Introduction
- Diabetes mellitus (DM) is one of the most prevalent chronic metabolic disorders worldwide and represents a major public health challenge.
- It is characterized by persistent hyperglycemia resulting from defects in insulin secretion, insulin action, or both.
- The disease affects millions of individuals globally and is associated with significant morbidity and mortality due to its long-term complications involving the cardiovascular system, kidneys, eyes, nerves, and other organs.
- The term “diabetes” is derived from the Greek word meaning “to pass through,” referring to excessive urination, while “mellitus” is derived from the Latin word for honey, indicating the sweet taste of urine observed in affected individuals.
- Historically, diabetes was diagnosed by observing symptoms such as excessive thirst, frequent urination, unexplained weight loss, and the presence of sugar in urine.
- However, advances in laboratory medicine have transformed the diagnosis and monitoring of diabetes from simple urine testing to highly sophisticated molecular and genetic investigations.
Glucose Homeostasis
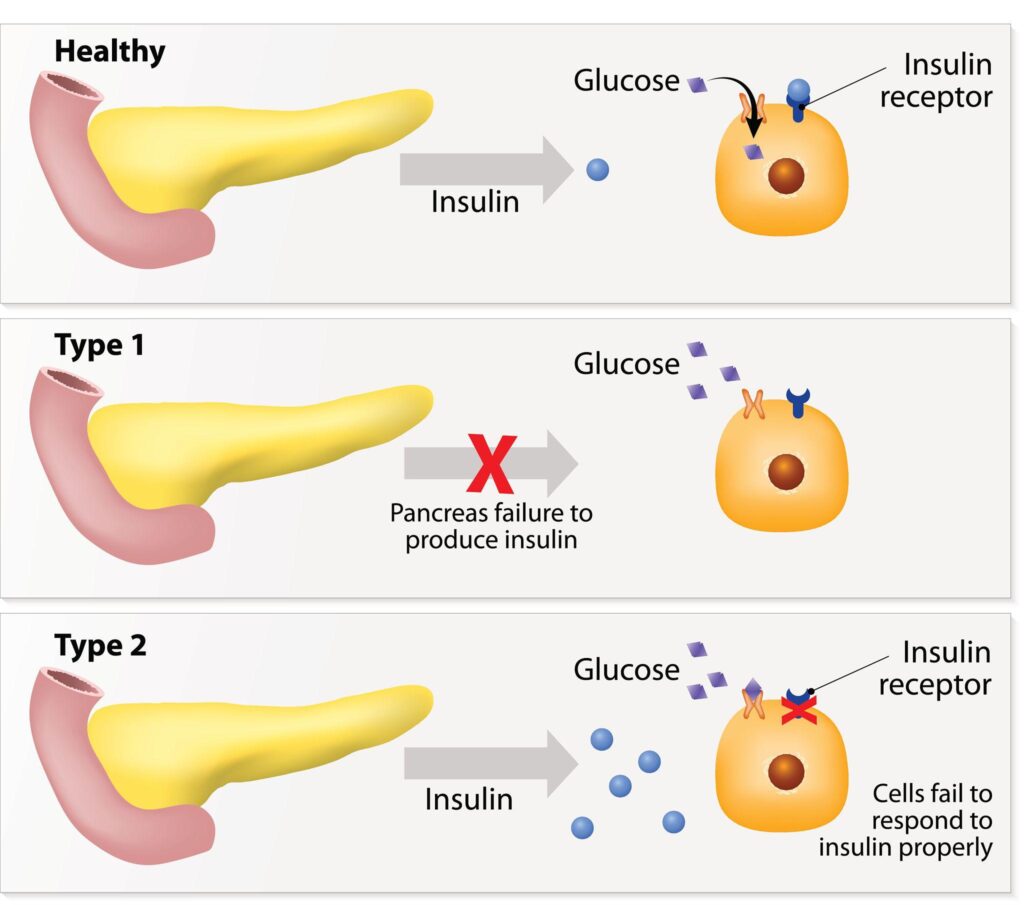
- Under normal physiological conditions, blood glucose concentration is maintained within a narrow range through a complex interaction between insulin and counter-regulatory hormones.
- Insulin, produced by the β-cells of the pancreatic islets of Langerhans, facilitates the uptake of glucose by peripheral tissues, promotes glycogen synthesis, and inhibits hepatic glucose production.
- Several hormones oppose the action of insulin and prevent hypoglycemia.
- These include glucagon, cortisol, growth hormone, and catecholamines.
- Together, these hormones maintain glucose homeostasis and ensure an adequate supply of energy to body tissues.
- Any disruption in this finely regulated system can lead to abnormal glucose metabolism and eventually diabetes mellitus.
Molecular Basis of Diabetes Mellitus
At the molecular level, diabetes mellitus is a heterogeneous group of disorders involving defects in insulin production, insulin signaling pathways, glucose transport mechanisms, and genetic regulation of metabolism.
Type 1 Diabetes Mellitus
- Type 1 diabetes mellitus (T1DM) is primarily an autoimmune disease characterized by immune-mediated destruction of pancreatic β-cells.
- Genetic susceptibility, particularly involving Human Leukocyte Antigen (HLA) genes on chromosome 6, plays a crucial role.
- Environmental triggers such as viral infections may initiate an autoimmune response leading to progressive β-cell destruction.
Autoantibodies commonly detected include:
- Glutamic Acid Decarboxylase Antibodies (GAD65)
- Insulin Autoantibodies (IAA)
- Islet Cell Antibodies (ICA)
- Insulinoma-Associated Antigen-2 Antibodies (IA-2)
- Zinc Transporter 8 Antibodies (ZnT8)
Loss of β-cell mass ultimately results in absolute insulin deficiency and dependence on exogenous insulin therapy.
Type 2 Diabetes Mellitus
- Type 2 diabetes mellitus (T2DM) accounts for approximately 90–95% of diabetes cases worldwide.
- It develops due to a combination of insulin resistance and progressive β-cell dysfunction.
At the cellular level, insulin resistance involves:
- Impaired insulin receptor signaling
- Defective phosphorylation of insulin receptor substrates
- Reduced translocation of GLUT-4 glucose transporters
- Increased inflammatory cytokines such as TNF-α and IL-6
- Mitochondrial dysfunction and oxidative stress
Initially, pancreatic β-cells compensate by increasing insulin secretion. However, chronic metabolic stress eventually leads to β-cell exhaustion and inadequate insulin production.
Genetic and Epigenetic Factors
- Recent studies have identified more than 400 genetic loci associated with diabetes susceptibility.
- Genes such as TCF7L2, PPARG, KCNJ11, SLC30A8, and FTO contribute to disease development.
- Epigenetic modifications, including DNA methylation, histone modifications, and microRNA regulation, are increasingly recognized as important factors influencing gene expression and disease progression. These molecular mechanisms provide the basis for future precision medicine approaches in diabetes management.
Laboratory Diagnosis
Because hyperglycemia may remain asymptomatic for years, laboratory investigations are essential for early detection, classification, monitoring, and prognostication of diabetes mellitus.
The objectives of laboratory testing include:
- Establishing the diagnosis of diabetes
- Identifying prediabetes and high-risk individuals
- Differentiating various forms of diabetes
- Monitoring glycemic control
- Detecting acute metabolic complications
- Evaluating chronic vascular complications
- Assessing therapeutic response
- Supporting personalized treatment strategies
Past: Historical Lab Diagnosis of DM
- The history of diabetes diagnosis spans more than 3,500 years and reflects the evolution of medical science from simple clinical observations to sophisticated biochemical testing.
- Long before the discovery of glucose, insulin, or modern laboratory instruments, physicians relied on characteristic symptoms and physical examination to identify individuals suffering from diabetes.
- The development of laboratory diagnosis has played a crucial role in improving the accuracy of diabetes detection and management.

Ancient Recognition of Diabetes
- The earliest descriptions of diabetes can be traced to ancient civilizations.
- Egyptian medical texts dating back to approximately 1550 BCE, particularly the Ebers Papyrus, described a condition characterized by excessive urination.
- Although the underlying cause was unknown, physicians recognized the abnormal loss of body fluids as a significant disease manifestation.
- Ancient Indian physicians, including Charaka and Sushruta (400–500 BCE), provided remarkably accurate descriptions of diabetes. They referred to the disease as Madhumeha, meaning “honey urine.”
- The diagnosis was often made by observing whether ants and insects were attracted to a patient’s urine. This observation represented one of the earliest methods of detecting glycosuria.
Clinical Diagnosis Before Laboratory Testing
For centuries, diabetes diagnosis depended primarily on clinical symptoms. Physicians relied on:
- Excessive thirst (polydipsia)
- Excessive urination (polyuria)
- Excessive hunger (polyphagia)
- Unexplained weight loss
- Fatigue and weakness
- Sweet-smelling urine
Since laboratory techniques were unavailable, diagnosis was often delayed until symptoms became severe. Consequently, many patients remained undiagnosed until advanced stages of the disease.
Urine Examination: The First Diagnostic Tool
- Before blood glucose measurements became possible, urine analysis served as the principal laboratory method for diagnosing diabetes.
Observation of Urine Characteristics
Physicians examined urine for:
- Volume
- Color
- Odor
- Specific gravity
- Presence of sweetness
Sweet-smelling urine was considered highly suggestive of diabetes. In some cases, physicians even tasted urine to determine whether it contained sugar. Although primitive by modern standards, this practice provided valuable diagnostic information.
Chemical Detection of Glucose in Urine
- The nineteenth century witnessed major advances in chemistry, leading to the development of laboratory tests capable of detecting reducing sugars in urine.
Trommer’s Test
- Developed in 1841 by Carl Trommer, this was among the earliest chemical methods used to detect glucose in urine.
Principle
- Glucose reduces cupric ions (Cu²⁺) to cuprous oxide (Cu₂O) in an alkaline medium.
Positive Result
- Formation of a red or orange precipitate indicated the presence of reducing sugars.
Limitations
- Poor sensitivity
- Interference by other reducing substances
- Difficulty in interpretation
Although largely obsolete today, Trommer’s test laid the foundation for future glucose detection methods.
Fehling’s Test
- Introduced by German chemist Hermann von Fehling in 1849, Fehling’s test became one of the most widely used methods for urine glucose estimation.
Principle
- The test employed an alkaline copper sulfate solution. When heated with urine containing glucose, the blue cupric ions were reduced to red cuprous oxide.
Procedure
- Fehling’s solution was mixed with urine.
- The mixture was heated.
- Formation of a brick-red precipitate indicated glucose.
Advantages
- More reliable than earlier methods.
- Simple and inexpensive.
Limitations
- Non-specific.
- Positive results could occur with other reducing substances such as fructose, lactose, uric acid, and certain drugs.
Despite these limitations, Fehling’s test remained a standard diagnostic method for several decades.
Benedict’s Test
- In 1908, Stanley Rossiter Benedict developed Benedict’s reagent, which became one of the most popular methods for detecting urinary glucose.
Principle
- Reducing sugars reduce copper sulfate in alkaline conditions, resulting in a color change proportional to glucose concentration.
Interpretation
| Color Change | Approximate Glucose Concentration |
|---|---|
| Blue | Negative |
| Green | Trace |
| Yellow | Moderate |
| Orange | High |
| Brick Red | Very High |
Advantages
- Easy to perform.
- Semi-quantitative.
- Suitable for routine clinical laboratories.
Limitations
- Could not distinguish glucose from other reducing sugars.
- Provided only an approximate estimate of glucose concentration.
For many years, Benedict’s test was widely used in hospitals, clinics, and teaching laboratories.
Measurement of Urine Specific Gravity
- As laboratory techniques improved, measurement of urine specific gravity became another supportive diagnostic tool.
Principle
- Diabetic patients often excrete large amounts of glucose in urine, increasing urine density.
Method
- A urinometer was used to determine specific gravity.
Significance
- High specific gravity in conjunction with polyuria and glycosuria strengthened the suspicion of diabetes.
- However, this method lacked specificity and could not independently establish the diagnosis.
Quantitative Urine Sugar Estimation
- By the early twentieth century, efforts were made to estimate the quantity of glucose excreted in urine.
Methods included:
- Copper reduction techniques
- Polarimetric measurements
- Fermentation methods
Although these methods improved accuracy, they remained labor-intensive and were gradually replaced by blood glucose measurements.
Blood Glucose Determination
- The greatest advancement in diabetes diagnosis occurred when blood glucose measurement became possible.
Early Blood Glucose Methods
- In the late nineteenth and early twentieth centuries, scientists developed methods to measure glucose directly in blood samples.
- One of the earliest techniques was the Folin-Wu method, introduced in 1919.
Folin-Wu Method
Principle
Proteins were precipitated from blood samples, and glucose was measured using copper reduction reactions.
Advantages
- Direct measurement of blood glucose.
- Greater accuracy than urine testing.
Limitations
- Labor-intensive.
- Required large blood volumes.
- Susceptible to interference.
Despite these challenges, blood glucose estimation revolutionized diabetes diagnosis.
Discovery of Insulin and Impact on Laboratory Testing
- The discovery of insulin in 1921 by Frederick Banting and Charles Best transformed diabetes management.
Following insulin therapy, laboratory testing became increasingly important for:
- Monitoring treatment response
- Adjusting insulin dosage
- Preventing complications
This development stimulated further improvements in glucose measurement techniques.
Clinitest Tablets
- In the mid-twentieth century, Clinitest tablets became widely used for home and clinical urine glucose testing.
Principle
- The tablet contained copper sulfate and alkaline reagents. When mixed with urine and water, a color-producing reaction occurred.
Advantages
- Convenient
- Portable
- Easy to perform
Limitations
- Measured urine glucose rather than blood glucose.
- Reflected past rather than current glycemic status.
- Could miss episodes of hypoglycemia.
Clinitest represented an important step toward patient self-monitoring before blood glucose meters became available.
Urine Ketone Testing
- As understanding of diabetic ketoacidosis expanded, urine ketone testing became an essential laboratory investigation.
Nitroprusside Reaction
- Ketone bodies reacted with sodium nitroprusside to produce a purple color.
Clinical Importance
Urine ketone testing helped detect:
- Diabetic ketoacidosis (DKA)
- Severe insulin deficiency
- Poor glycemic control
This test significantly improved the management of acute diabetic emergencies.
Limitations of Historical Diagnostic Methods
Although historical diagnostic methods were invaluable during their time, they possessed several limitations:
- Poor sensitivity and specificity
- Dependence on urine glucose rather than blood glucose
- Inability to detect early disease
- Lack of standardization
- Delayed diagnosis
- Inability to monitor short-term glycemic changes accurately
Many patients remained undiagnosed until complications developed, highlighting the need for more precise laboratory techniques.
Present: Current Lab Investigations of DM
- The diagnosis and management of diabetes mellitus have undergone remarkable advancements over the past few decades.
- Modern laboratory investigations enable accurate diagnosis, classification, monitoring, and assessment of complications associated with diabetes.
- Unlike historical methods that relied primarily on urine glucose detection, current diagnostic approaches focus on direct measurement of blood glucose and biomarkers reflecting long-term glycemic control.
- Laboratory investigations play a central role in identifying diabetes at an early stage, monitoring treatment efficacy, preventing complications, and guiding individualized therapeutic decisions.
- International organizations such as the American Diabetes Association and the World Health Organization have established standardized diagnostic criteria based on laboratory findings.
Blood Glucose Measurement
Blood glucose estimation remains the cornerstone of diabetes diagnosis.
Fasting Plasma Glucose (FPG)
- Fasting plasma glucose is one of the most widely used tests for diagnosing diabetes.
Principle
- The test measures plasma glucose concentration after at least 8–12 hours of fasting.
Diagnostic Criteria
| Category | Fasting Plasma Glucose |
|---|---|
| Normal | <100 mg/dL (<5.6 mmol/L) |
| Prediabetes | 100–125 mg/dL (5.6–6.9 mmol/L) |
| Diabetes Mellitus | ≥126 mg/dL (≥7.0 mmol/L) |
Advantages
- Simple and inexpensive
- Highly standardized
- Good reproducibility
- Suitable for mass screening
Limitations
- Requires overnight fasting
- May miss postprandial hyperglycemia
Random Plasma Glucose (RPG)
- Random plasma glucose can be measured at any time regardless of food intake.
Diagnostic Criterion
- A random plasma glucose level of: ≥200 mg/dL (11.1 mmol/L)
- along with classic symptoms of hyperglycemia is diagnostic of diabetes.
Clinical Utility
- Emergency diagnosis
- Symptomatic patients
- Hospital settings
Postprandial Blood Glucose (PPBG)
- Postprandial blood glucose is measured two hours after a meal.
Significance
- Detects postprandial hyperglycemia
- Assesses glucose handling after food intake
- Evaluates treatment effectiveness
Normal Value
Less than 140 mg/dL after two hours.
Oral Glucose Tolerance Test (OGTT)
- The Oral Glucose Tolerance Test evaluates the body’s ability to metabolize glucose.
Procedure
- Overnight fasting for 8–12 hours.
- Fasting blood sample collected.
- Administration of 75 g anhydrous glucose dissolved in water.
- Blood glucose measured after 2 hours.
Interpretation
| Category | 2-Hour Plasma Glucose |
|---|---|
| Normal | <140 mg/dL |
| Prediabetes (IGT) | 140–199 mg/dL |
| Diabetes Mellitus | ≥200 mg/dL |
Clinical Applications
- Confirmation of diabetes
- Diagnosis of gestational diabetes
- Detection of impaired glucose tolerance
- Identification of early abnormalities in glucose metabolism
Advantages
- Highly sensitive
- Detects postprandial abnormalities
Limitations
- Time-consuming
- Requires patient preparation
- Poor reproducibility compared with HbA1c
Glycated Hemoglobin (HbA1c)
- HbA1c has become one of the most important laboratory markers in diabetes care.
Biochemical Basis
- Glucose binds non-enzymatically to hemoglobin within red blood cells, forming glycated hemoglobin (HbA1c).
- Since erythrocytes survive approximately 120 days, HbA1c reflects average blood glucose over the preceding 2–3 months.
Diagnostic Criteria
| HbA1c (%) | Interpretation |
|---|---|
| <5.7 | Normal |
| 5.7–6.4 | Prediabetes |
| ≥6.5 | Diabetes Mellitus |
Clinical Importance
- Diagnosis of diabetes
- Long-term glycemic monitoring
- Assessment of treatment efficacy
- Prediction of complications
Advantages
- No fasting required
- Reflects long-term glucose control
- Convenient for patients
Limitations
HbA1c may be inaccurate in:
- Hemolytic anemia
- Hemoglobinopathies
- Chronic kidney disease
- Recent blood transfusion
- Pregnancy
Continuous Glucose Monitoring (CGM)
- Continuous Glucose Monitoring represents a major advancement in diabetes management.
Principle
A subcutaneous sensor measures interstitial glucose levels continuously throughout the day and night.
Benefits
- Real-time glucose monitoring
- Detection of nocturnal hypoglycemia
- Assessment of glucose variability
- Improved glycemic control
Important Parameters
- Time in Range (TIR)
- Time Above Range (TAR)
- Time Below Range (TBR)
- Glucose Management Indicator (GMI)
CGM is increasingly used in both Type 1 and Type 2 diabetes.
Fructosamine
- Fructosamine measures glycated serum proteins, primarily albumin.
Significance
- Reflects average blood glucose over the previous 2–3 weeks.
Clinical Uses
- Monitoring recent glycemic changes
- Assessment during pregnancy
- Situations where HbA1c is unreliable
Advantages
- Short-term glycemic assessment
- Rapid response to treatment changes
Insulin Assay
- Measurement of circulating insulin helps evaluate pancreatic β-cell function.
Clinical Applications
- Differentiating diabetes types
- Investigation of insulin resistance
- Evaluation of hypoglycemia
- Research studies
Methodology
- Immunoassays
- Chemiluminescent assays
- ELISA-based methods
C-Peptide Assay
- C-peptide is released in equimolar amounts with endogenous insulin.
Importance
- Provides a reliable measure of endogenous insulin production.
Clinical Applications
- Distinguishing Type 1 from Type 2 diabetes
- Assessment of residual β-cell function
- Evaluation of insulin therapy
Interpretation
- Low C-peptide → Type 1 diabetes
- Normal/high C-peptide → Type 2 diabetes or insulin resistance
Autoantibody Testing
- Autoimmune markers are important for diagnosing Type 1 diabetes.
Major Autoantibodies
- Glutamic Acid Decarboxylase Antibody (GAD65)
Most common autoantibody in Type 1 diabetes.
- Islet Cell Antibody (ICA)
Targets pancreatic islet cells.
- Insulin Autoantibody (IAA)
Common in children with newly diagnosed Type 1 diabetes.
- Insulinoma-Associated Antigen-2 Antibody (IA-2)
Indicates autoimmune β-cell destruction.
- Zinc Transporter 8 Antibody (ZnT8)
- Improves diagnostic sensitivity for autoimmune diabetes.
Clinical Utility
- Early diagnosis of Type 1 diabetes
- Prediction of disease risk
- Differentiation from Type 2 diabetes
Ketone Body Testing
Ketone testing is crucial in diabetic emergencies.
Ketone Bodies Measured
- Acetoacetate
- β-Hydroxybutyrate
- Acetone
Methods
- Urine ketone strips
- Blood ketone meters
- Laboratory enzymatic assays
Clinical Importance
- Detection of diabetic ketoacidosis (DKA)
- Monitoring treatment response
Urine Examination
- Although no longer used for primary diagnosis, urine testing remains valuable.
Urinary Glucose
- May indicate poor glycemic control.
Urinary Ketones
- Suggest ketosis or ketoacidosis.
Urinary Albumin
- Early marker of diabetic nephropathy.
Urine Albumin-to-Creatinine Ratio (UACR)
- Microalbuminuria is the earliest clinical sign of diabetic kidney disease.
Interpretation
| UACR | Interpretation |
|---|---|
| <30 mg/g | Normal |
| 30–300 mg/g | Microalbuminuria |
| >300 mg/g | Macroalbuminuria |
Clinical Importance
- Early detection of nephropathy
- Monitoring kidney damage progression
Renal Function Tests
Diabetes is a leading cause of chronic kidney disease.
Investigations
- Serum creatinine
- Blood urea nitrogen (BUN)
- Estimated Glomerular Filtration Rate (eGFR)
Clinical Significance
- Assessment of renal function
- Monitoring diabetic nephropathy
- Drug dose adjustment
Lipid Profile
Diabetic dyslipidemia significantly increases cardiovascular risk.
Parameters
- Total cholesterol
- LDL cholesterol
- HDL cholesterol
- Triglycerides
- Non-HDL cholesterol
Importance
- Cardiovascular risk assessment
- Treatment monitoring
Liver Function Tests
The association between diabetes and non-alcoholic fatty liver disease (NAFLD) makes liver assessment important.
Parameters
- ALT
- AST
- ALP
- GGT
- Bilirubin
Clinical Significance
- Detection of fatty liver disease
- Monitoring metabolic syndrome
Emerging Biomarkers in Current Practice
Several novel biomarkers are increasingly being evaluated in specialized laboratories:
- High-sensitivity C-reactive protein (hs-CRP)
- Adiponectin
- Leptin
- Interleukin-6 (IL-6)
- Tumor Necrosis Factor-α (TNF-α)
- Oxidative stress markers
These biomarkers may provide additional information regarding inflammation, insulin resistance, and cardiovascular risk.
Future: Emerging Lab Diagnostics of DM
- The future of diabetes diagnostics is being shaped by rapid advances in molecular biology, genomics, bioinformatics, nanotechnology, and artificial intelligence.
- While current diagnostic methods such as fasting plasma glucose, oral glucose tolerance tests, and HbA1c measurements remain highly effective, they primarily detect diabetes after significant metabolic abnormalities have already developed.
- Emerging laboratory technologies aim to identify individuals at risk much earlier, predict disease progression, monitor treatment responses in real time, and enable personalized therapeutic strategies.
Need for Advanced Diagnostic Approaches
Current laboratory tests have several limitations:
- They often detect disease after substantial β-cell dysfunction has occurred.
- They provide limited information regarding disease mechanisms.
- They cannot accurately predict individual treatment responses.
- They offer minimal insight into genetic susceptibility.
- They may not identify high-risk individuals before hyperglycemia develops.
Future diagnostics aim to overcome these limitations through precision medicine approaches.
Genetic Testing and Genomic Diagnostics
Genetic studies have revealed that diabetes is influenced by numerous susceptibility genes.
Role of Genetic Testing
Genetic testing can identify inherited risk factors associated with:
- Type 1 diabetes mellitus
- Type 2 diabetes mellitus
- Monogenic diabetes
- Maturity-Onset Diabetes of the Young (MODY)
- Neonatal diabetes
Important Diabetes-Associated Genes
Several genes have been implicated in diabetes susceptibility, including:
- TCF7L2
- PPARG
- KCNJ11
- HNF1A
- HNF4A
- GCK
- SLC30A8
- FTO
Future diagnostic panels may screen these genes to identify individuals at high risk before disease onset.
Clinical Applications
- Early risk prediction
- Family screening
- Disease classification
- Selection of targeted therapies
- Personalized preventive interventions
Epigenetic Biomarkers
- Epigenetics refers to heritable changes in gene expression that occur without altering the DNA sequence.
Major Epigenetic Mechanisms
- DNA methylation
- Histone modification
- Chromatin remodeling
- Non-coding RNA regulation
Role in Diabetes
- Environmental factors such as obesity, diet, physical inactivity, and stress can induce epigenetic changes that contribute to insulin resistance and β-cell dysfunction.
Future Diagnostic Potential
Epigenetic biomarkers may:
- Predict diabetes risk
- Detect disease before hyperglycemia develops
- Monitor disease progression
- Assess therapeutic response
These biomarkers are particularly attractive because many epigenetic changes are potentially reversible.
MicroRNA-Based Diagnostics
MicroRNAs (miRNAs) are small non-coding RNA molecules that regulate gene expression.
Importance in Diabetes
Specific microRNAs influence:
- Insulin secretion
- Insulin sensitivity
- β-cell survival
- Inflammatory pathways
- Glucose metabolism
Potential Diagnostic Uses
- Early detection of diabetes
- Prediction of complications
- Monitoring treatment response
- Assessment of cardiovascular risk
Because microRNAs can be measured in blood samples, they represent promising non-invasive biomarkers.
Proteomics
- Proteomics involves the large-scale study of proteins expressed in cells, tissues, and biological fluids.
Significance
- Proteins directly reflect ongoing physiological and pathological processes.
Applications in Diabetes
Proteomic analysis may identify:
- Early biomarkers of insulin resistance
- Markers of β-cell dysfunction
- Predictors of diabetic complications
- Novel therapeutic targets
Future laboratory platforms may use protein signatures to detect diabetes years before clinical diagnosis.
Metabolomics
- Metabolomics examines small molecules produced during metabolism.
Importance
- Changes in metabolite profiles often occur before clinical disease becomes apparent.
Potential Biomarkers
Studies have identified alterations in:
- Branched-chain amino acids
- Acylcarnitines
- Fatty acids
- Organic acids
- Lipid metabolites
Clinical Applications
Metabolomic profiling may:
- Predict future diabetes development
- Assess disease severity
- Identify therapeutic targets
- Monitor metabolic responses to treatment
Artificial Intelligence and Machine Learning
- Artificial Intelligence (AI) is expected to play an increasingly important role in diabetes diagnostics.
Applications
AI systems can analyze:
- Laboratory results
- Continuous glucose monitoring data
- Genetic information
- Electronic health records
- Imaging studies
Benefits
- Improved diagnostic accuracy
- Earlier disease prediction
- Personalized risk assessment
- Automated interpretation of complex datasets
Machine learning algorithms may identify subtle patterns that are difficult for humans to recognize.
Wearable Biosensors
- Wearable technology is rapidly transforming glucose monitoring.
Current Developments
Modern biosensors can continuously measure:
- Glucose levels
- Physical activity
- Heart rate
- Sleep patterns
Future Potential
- Advanced wearable devices may simultaneously monitor multiple biomarkers and provide personalized health recommendations in real time.
Non-Invasive Glucose Monitoring
- Traditional glucose monitoring requires finger-prick blood sampling, which can be uncomfortable and reduce patient compliance.
Emerging Technologies
Researchers are developing devices that measure glucose through:
- Sweat
- Tears
- Saliva
- Interstitial fluid
- Skin spectroscopy
- Optical sensing technologies
Advantages
- Painless monitoring
- Improved patient adherence
- Continuous glucose assessment
- Reduced infection risk
Non-invasive glucose monitoring represents one of the most anticipated advancements in diabetes care.
Nanotechnology-Based Diagnostics
- Nanotechnology enables the development of highly sensitive biosensors capable of detecting minute concentrations of biological markers.
Applications
Nanoparticle-based sensors may be used for:
- Glucose detection
- Insulin measurement
- Inflammatory biomarker analysis
- Detection of diabetic complications
Advantages
- High sensitivity
- Rapid results
- Small sample volume
- Point-of-care testing capability
Nanodiagnostics may significantly enhance early disease detection.
Multi-Omics Approaches
- Future diabetes diagnostics are likely to integrate multiple biological datasets.
Components of Multi-Omics Analysis
- Genomics
- Transcriptomics
- Epigenomics
- Proteomics
- Metabolomics
Benefits
- This comprehensive approach can provide a detailed understanding of disease mechanisms and individual patient characteristics.
Precision Medicine in Diabetes
The ultimate goal of emerging laboratory diagnostics is precision medicine.
Precision Medicine Involves
- Individual risk prediction
- Early disease detection
- Personalized treatment selection
- Continuous monitoring
- Prevention of complications
Instead of treating all patients similarly, precision medicine tailors healthcare decisions according to each individual’s genetic, molecular, and clinical profile.
Challenges and Future Directions
Despite promising advances, several challenges remain:
- High cost of advanced technologies
- Limited accessibility in developing countries
- Need for standardization
- Ethical concerns regarding genetic data
- Large-scale validation studies
Continued research and technological development will be essential before these approaches become routine clinical practice.