Introduction
- Lipids are among the most important biomolecules in the human body.
- They serve as major sources of energy, structural components of cell membranes, precursors of hormones, and essential molecules for numerous physiological functions.
- Despite their vital roles, abnormalities in lipid metabolism have become increasingly common due to sedentary lifestyles, unhealthy dietary habits, obesity, and metabolic disorders.
- The term “lipid profile” is often associated with cardiovascular health because blood lipids directly influence the development of atherosclerosis, coronary artery disease, stroke, and peripheral vascular disease.
- However, lipids are much more than cardiovascular risk factors.
- They are fundamental to cellular function, energy storage, nerve conduction, hormone synthesis, and immune regulation.
What Are Lipids?
- Lipids are a diverse group of organic compounds that are insoluble in water but soluble in organic solvents.
- They consist primarily of carbon, hydrogen, and oxygen atoms.
The major categories of lipids found in the human body include:
Triglycerides
- Triglycerides are the body’s primary storage form of energy.
- They consist of one glycerol molecule attached to three fatty acid molecules.
- Excess calories from carbohydrates, fats, or proteins are converted into triglycerides and stored in adipose tissue.
- During periods of fasting or increased energy demand, triglycerides are broken down to release energy.
Cholesterol
Cholesterol is a waxy, fat-like substance present in every cell of the body. It is required for:
- Cell membrane formation
- Steroid hormone synthesis
- Vitamin D production
- Bile acid formation
- Maintenance of membrane fluidity
Although cholesterol is essential for life, excessive accumulation can contribute to cardiovascular disease.
Phospholipids
- Phospholipids are major structural components of cell membranes.
- Their unique structure allows them to form lipid bilayers, creating a barrier between intracellular and extracellular environments.
Free Fatty Acids
- Free fatty acids circulate in the bloodstream and serve as important energy substrates for muscles, the heart, and other tissues.
Biological Functions of Lipids
Lipids perform numerous functions essential for survival.
1. Energy Storage
- The most important role of lipids is long-term energy storage.
- Triglycerides stored in adipose tissue serve as the body’s energy reserve.
- During periods of fasting, starvation, prolonged exercise, or illness, these stored fats are mobilized and utilized for energy production.
- Fat provides approximately 9 kcal per gram, making it more energy-dense than carbohydrates or proteins, which provide only 4 kcal per gram.
- This high energy density allows humans to store large amounts of energy in a relatively compact form.
2. Structural Components of Cell Membranes
Every cell in the body is surrounded by a plasma membrane composed primarily of phospholipids and cholesterol.
These lipids:
- Maintain membrane integrity
- Regulate membrane fluidity
- Facilitate cellular communication
- Control transport of substances across membranes
Without lipids, cells would lose their structural stability and functional organization.
3. Hormone Synthesis
Cholesterol serves as the precursor for several important hormones, including:
- Cortisol
- Aldosterone
- Testosterone
- Estrogen
- Progesterone
These hormones regulate growth, reproduction, metabolism, electrolyte balance, and stress responses.
4. Absorption of Fat-Soluble Vitamins
Dietary lipids facilitate absorption of:
- Vitamin A
- Vitamin D
- Vitamin E
- Vitamin K
Defects in fat digestion or absorption may lead to deficiencies of these vitamins despite adequate dietary intake.
5. Protection and Insulation
Adipose tissue provides:
- Mechanical protection for internal organs
- Thermal insulation
- Cushioning against physical injury
This protective role is particularly important around the kidneys, eyes, and abdominal organs.
Lipid Profile and Cardiovascular Disease
- Cardiovascular disease (CVD) remains one of the leading causes of death worldwide.
- A major contributor to the development of cardiovascular disorders is an abnormal lipid profile, particularly elevated levels of low-density lipoprotein (LDL) cholesterol and triglycerides, along with reduced levels of high-density lipoprotein (HDL) cholesterol.
- Because lipid abnormalities often develop silently without noticeable symptoms, a lipid profile serves as one of the most valuable tools for identifying individuals at increased cardiovascular risk.
How Lipids Affect Blood Vessels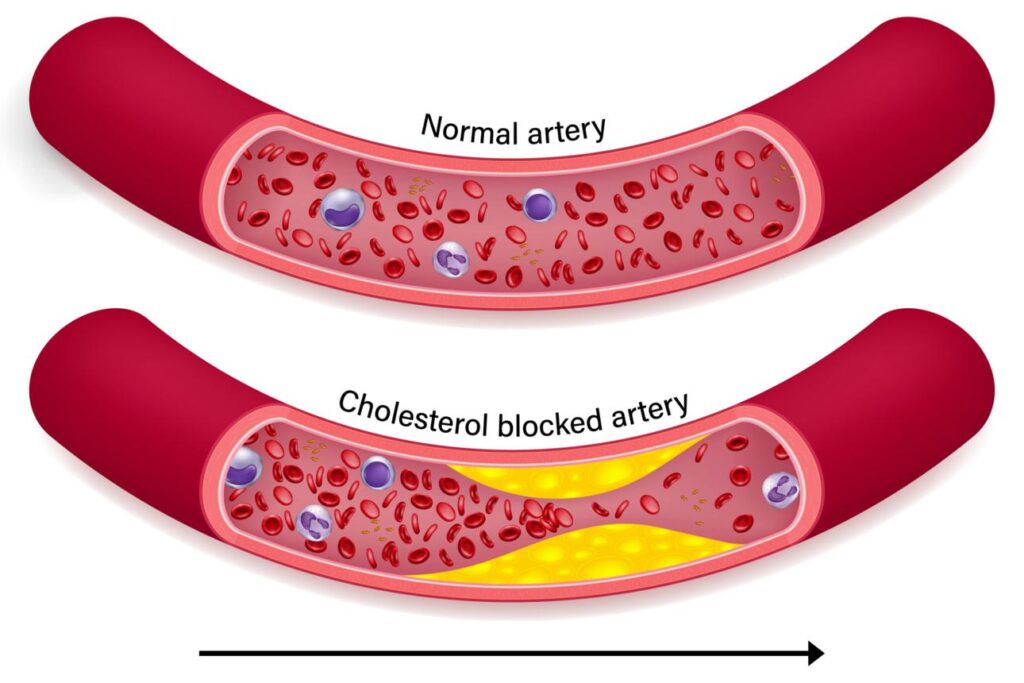
- The inner lining of blood vessels, known as the endothelium, normally provides a smooth surface that allows blood to flow freely.
- However, factors such as hypertension, smoking, diabetes mellitus, obesity, chronic inflammation, and elevated LDL cholesterol can damage this protective lining.
- When LDL cholesterol levels remain elevated for prolonged periods, LDL particles penetrate the arterial wall and accumulate beneath the endothelium.
- These trapped LDL particles undergo oxidation, triggering an inflammatory response.
- Macrophages migrate to the site and engulf oxidized LDL, transforming into foam cells.
- The accumulation of foam cells forms fatty streaks, which represent the earliest visible lesions of atherosclerosis.
- Over time, additional cholesterol, inflammatory cells, connective tissue, and calcium deposits accumulate, resulting in the formation of an atherosclerotic plaque.
- As plaques enlarge, they narrow the arterial lumen and reduce blood flow to vital organs.
The Role of LDL Cholesterol
- LDL cholesterol is often referred to as the “bad cholesterol” because it plays a central role in atherosclerotic plaque formation.
- LDL transports cholesterol from the liver to peripheral tissues where it is used for membrane synthesis and hormone production.
- However, excessive LDL promotes cholesterol deposition within arterial walls.
Persistently elevated LDL cholesterol is associated with:
- Coronary artery disease
- Myocardial infarction (heart attack)
- Ischemic stroke
- Peripheral arterial disease
- Sudden cardiac death
Numerous clinical studies have demonstrated that lowering LDL cholesterol significantly reduces the risk of cardiovascular events.
Protective Effects of HDL Cholesterol
- High-density lipoprotein (HDL) cholesterol performs the opposite function of LDL.
- HDL removes excess cholesterol from tissues and blood vessel walls and transports it back to the liver for processing and excretion.
- This process is known as reverse cholesterol transport.
HDL provides cardiovascular protection through several mechanisms:
- Removal of excess cholesterol from arteries
- Antioxidant activity
- Anti-inflammatory effects
- Improvement of endothelial function
- Reduction of plaque progression
Individuals with higher HDL levels generally have a lower risk of cardiovascular disease.
Triglycerides and Cardiovascular Risk
- Although cholesterol receives most of the attention, elevated triglycerides also contribute to cardiovascular disease.
- Increased triglyceride concentrations are commonly associated with obesity, diabetes mellitus, metabolic syndrome, insulin resistance, and sedentary lifestyles.
High triglyceride levels often occur together with:
- Reduced HDL cholesterol
- Increased small dense LDL particles
- Insulin resistance
- Chronic inflammation
This combination substantially increases cardiovascular risk.
Atherosclerosis: The Link Between Lipids and Heart Disease
Atherosclerosis is a chronic progressive disease characterized by the accumulation of lipid-rich plaques within arterial walls.
The process typically follows these stages:
- Endothelial injury
- LDL infiltration into arterial walls
- Oxidation of LDL particles
- Recruitment of inflammatory cells
- Foam cell formation
- Fatty streak development
- Plaque growth and calcification
- Plaque rupture and thrombosis
The disease progresses slowly over many years and may remain asymptomatic until a major cardiovascular event occurs.
Coronary Artery Disease
When atherosclerotic plaques develop in coronary arteries, blood supply to the heart muscle becomes restricted. This condition is known as coronary artery disease (CAD).
Clinical manifestations include:
- Chest pain (angina pectoris)
- Shortness of breath
- Fatigue
- Heart attack
- Heart failure
CAD is one of the most common consequences of dyslipidemia.
Stroke and Cerebrovascular Disease
- Atherosclerotic plaques can also develop in arteries supplying the brain.
- Plaque rupture or arterial blockage can interrupt cerebral blood flow and result in an ischemic stroke.
- Abnormal lipid profiles are recognized as important risk factors for cerebrovascular disease and stroke-related mortality.
Peripheral Arterial Disease
Atherosclerosis may affect arteries supplying the legs and other peripheral tissues. Reduced blood flow can lead to:
- Leg pain during walking (claudication)
- Delayed wound healing
- Tissue ischemia
- Gangrene in severe cases
Patients with peripheral arterial disease frequently exhibit abnormal lipid profiles.
Why Lipid Profile Testing Is Important
The lipid profile helps identify individuals at increased risk of cardiovascular disease long before symptoms appear. Early detection of dyslipidemia allows implementation of preventive measures such as:
- Dietary modification
- Weight management
- Increased physical activity
- Smoking cessation
- Control of diabetes and hypertension
- Lipid-lowering therapy when required
By identifying risk factors at an early stage, lipid profile testing plays a crucial role in reducing cardiovascular morbidity and mortality.
Lipid Profile in Diabetes Mellitus
- Diabetes mellitus is one of the most common metabolic disorders worldwide and is characterized by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both.
- In addition to disturbances in carbohydrate metabolism, diabetes profoundly affects lipid metabolism, leading to characteristic abnormalities in the lipid profile.
- These lipid abnormalities, collectively known as diabetic dyslipidemia, significantly increase the risk of cardiovascular disease and contribute to the development of diabetic complications.
- Cardiovascular disease is the leading cause of morbidity and mortality among individuals with diabetes.
- Therefore, evaluation of the lipid profile is an essential component of diabetes management and risk assessment.
Relationship Between Insulin and Lipid Metabolism
Insulin plays a central role in regulating lipid metabolism. Under normal conditions, insulin:
- Inhibits lipolysis in adipose tissue
- Promotes triglyceride storage
- Reduces the release of free fatty acids into circulation
- Enhances lipid utilization by tissues
- Regulates hepatic lipoprotein synthesis
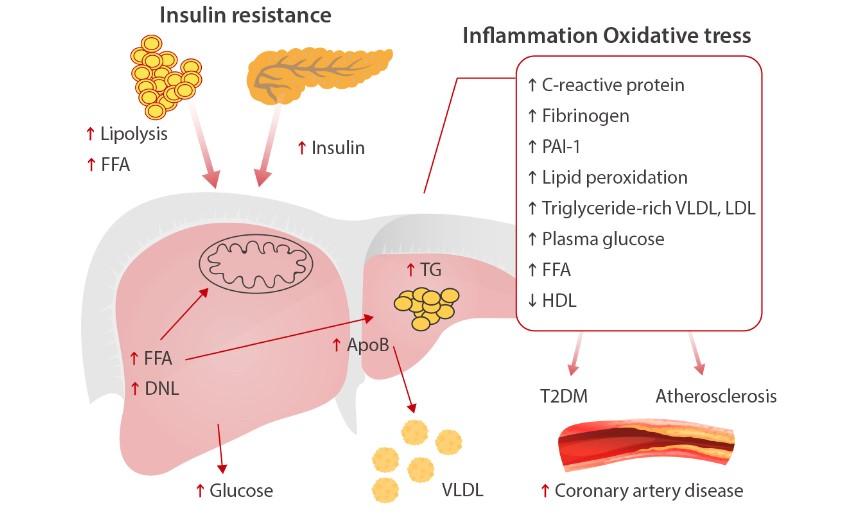
When insulin is deficient or when tissues become resistant to insulin, these regulatory mechanisms are disrupted. As a result, excessive amounts of free fatty acids are released from adipose tissue and transported to the liver, where they stimulate increased triglyceride synthesis and lipoprotein production.
Diabetic Dyslipidemia
The typical lipid abnormalities observed in diabetes mellitus include:
- Elevated triglycerides
- Increased very low-density lipoprotein (VLDL)
- Reduced high-density lipoprotein (HDL) cholesterol
- Increased concentration of small dense low-density lipoprotein (LDL) particles
This pattern is commonly referred to as diabetic dyslipidemia and is particularly common in individuals with type 2 diabetes mellitus.
Unlike ordinary LDL particles, small dense LDL particles are more atherogenic because they:
- Easily penetrate arterial walls
- Remain in circulation longer
- Are more susceptible to oxidation
- Promote plaque formation
Consequently, diabetic patients may develop cardiovascular disease even when total cholesterol levels appear relatively normal.
Elevated Triglycerides in Diabetes
- One of the most common lipid abnormalities in diabetes is hypertriglyceridemia.
- Insulin resistance increases the breakdown of stored triglycerides in adipose tissue, releasing large quantities of free fatty acids into the bloodstream.
- The liver utilizes these fatty acids to synthesize triglycerides and packages them into VLDL particles.
- As hepatic VLDL production increases, plasma triglyceride concentrations rise.
Persistent hypertriglyceridemia contributes to:
- Endothelial dysfunction
- Inflammation
- Atherosclerosis
- Increased cardiovascular risk
In severe cases, markedly elevated triglyceride levels may predispose patients to acute pancreatitis.
Reduced HDL Cholesterol
- HDL cholesterol is often called the “good cholesterol” because it removes excess cholesterol from peripheral tissues and transports it back to the liver.
- In diabetes mellitus, HDL concentrations are frequently reduced.
- Lower HDL levels impair reverse cholesterol transport, allowing cholesterol to accumulate within blood vessel walls.
Reduced HDL cholesterol is associated with:
- Accelerated atherosclerosis
- Coronary artery disease
- Stroke
- Peripheral vascular disease
The combination of elevated triglycerides and low HDL cholesterol is considered a hallmark of diabetic dyslipidemia.
LDL Cholesterol and Diabetes
Although LDL cholesterol levels may not always be markedly elevated in diabetic patients, the quality of LDL particles changes significantly.
Diabetes promotes the formation of:
- Small dense LDL particles
- Glycated LDL particles
- Oxidized LDL particles
These modified LDL particles are particularly harmful because they readily infiltrate arterial walls and initiate inflammatory responses.
Thus, diabetic patients often experience increased cardiovascular risk despite apparently acceptable LDL cholesterol concentrations.
Lipid Profile and Cardiovascular Risk in Diabetes
Individuals with diabetes are two to four times more likely to develop cardiovascular disease than non-diabetic individuals.
Several factors contribute to this increased risk:
- Hyperglycemia
- Insulin resistance
- Dyslipidemia
- Hypertension
- Chronic inflammation
- Endothelial dysfunction
The combined effect of these abnormalities accelerates the development of atherosclerosis.
Atherosclerotic plaque formation in diabetic patients may affect:
- Coronary arteries
- Cerebral arteries
- Peripheral arteries
- Renal blood vessels
As a result, diabetic individuals are at increased risk of:
- Myocardial infarction
- Stroke
- Peripheral arterial disease
- Chronic kidney disease
Lipid Profile and Diabetic Complications
- Abnormal lipid metabolism contributes not only to macrovascular complications but also to microvascular damage.
Several studies suggest that dyslipidemia may influence the progression of:
- Diabetic Nephropathy – Lipid accumulation within renal tissues may accelerate kidney damage and worsen renal function.
- Diabetic Retinopathy – Abnormal lipid concentrations have been associated with retinal vascular damage and the development of retinal exudates.
- Diabetic Neuropathy – Dyslipidemia may contribute to nerve injury through oxidative stress and microvascular dysfunction.
Therefore, maintaining a healthy lipid profile is important for preventing both cardiovascular and microvascular complications of diabetes.
Importance of Lipid Monitoring in Diabetes
Regular lipid profile assessment allows healthcare professionals to:
- Evaluate cardiovascular risk
- Detect diabetic dyslipidemia
- Monitor disease progression
- Assess response to lifestyle modifications
- Guide therapeutic interventions
Because lipid abnormalities often remain asymptomatic, routine monitoring plays a vital role in preventive healthcare.
Lipid Profile in Obesity and Metabolic Syndrome
- Obesity and metabolic syndrome are among the most significant public health challenges of the modern era.
- The increasing prevalence of sedentary lifestyles, unhealthy dietary habits, and reduced physical activity has contributed to a dramatic rise in obesity worldwide.
- These conditions are closely associated with disturbances in lipid metabolism, making lipid profile assessment an essential tool for evaluating metabolic health and cardiovascular risk.
Understanding Obesity and Lipid Metabolism
- Adipose tissue is not merely a storage site for excess fat.
- It functions as an active endocrine organ that produces numerous hormones, cytokines, and inflammatory mediators that influence metabolism throughout the body.
- In healthy individuals, adipose tissue stores excess energy in the form of triglycerides and releases fatty acids when energy is required.
- However, in obesity, particularly central or abdominal obesity, adipose tissue becomes metabolically dysfunctional.
This dysfunction results in:
- Increased release of free fatty acids (FFAs)
- Chronic inflammation
- Insulin resistance
- Altered adipokine secretion
- Enhanced hepatic lipid synthesis
These changes significantly affect the lipid profile and contribute to the development of cardiovascular disease.
Characteristic Lipid Profile Changes in Obesity
Individuals with obesity commonly exhibit a distinct pattern of lipid abnormalities known as atherogenic dyslipidemia.
The characteristic features include:
- Elevated triglycerides
- Increased very low-density lipoprotein (VLDL)
- Reduced high-density lipoprotein (HDL) cholesterol
- Increased small dense low-density lipoprotein (LDL) particles
This lipid pattern is strongly associated with accelerated atherosclerosis and increased cardiovascular risk.
Elevated Triglycerides
- One of the earliest lipid abnormalities observed in obesity is hypertriglyceridemia.
- Excess adipose tissue releases large quantities of free fatty acids into the bloodstream.
- These fatty acids are transported to the liver, where they are converted into triglycerides and packaged into VLDL particles.
- As hepatic VLDL production increases, plasma triglyceride levels rise.
Elevated triglycerides contribute to:
- Endothelial dysfunction
- Vascular inflammation
- Insulin resistance
- Increased cardiovascular risk
Persistent hypertriglyceridemia is frequently observed in individuals with central obesity.
Reduced HDL Cholesterol
- HDL cholesterol plays a protective role by removing excess cholesterol from peripheral tissues and transporting it back to the liver through reverse cholesterol transport.
- In obesity, HDL cholesterol levels are often reduced because increased triglyceride-rich lipoproteins alter HDL metabolism.
Low HDL cholesterol levels result in:
- Reduced cholesterol clearance
- Enhanced plaque formation
- Increased risk of coronary artery disease
- Greater susceptibility to cardiovascular events
The combination of elevated triglycerides and reduced HDL cholesterol is considered a hallmark of obesity-related dyslipidemia.
Small Dense LDL Particles
- Although total LDL cholesterol may not always be markedly elevated in obese individuals, the composition of LDL particles often changes.
Obesity promotes the formation of small dense LDL particles, which are more harmful than normal LDL particles because they:
- Penetrate arterial walls more easily
- Remain longer in circulation
- Undergo oxidation more readily
- Accelerate atherosclerotic plaque formation
Consequently, cardiovascular risk may be increased even when LDL cholesterol concentrations appear relatively normal.
Metabolic Syndrome and Lipid Profile
- Metabolic syndrome is a cluster of interconnected metabolic abnormalities that significantly increase the risk of cardiovascular disease and type 2 diabetes mellitus.
The syndrome is characterized by the presence of several metabolic disturbances, including:
- Central obesity
- Insulin resistance
- Hyperglycemia
- Hypertension
- Dyslipidemia
Among these features, dyslipidemia plays a central role in the development of cardiovascular complications.
Pathophysiology of Dyslipidemia in Metabolic Syndrome
- Insulin resistance is considered the primary underlying mechanism responsible for lipid abnormalities in metabolic syndrome.
When tissues become resistant to insulin:
- Lipolysis in adipose tissue increases
- Free fatty acid release rises
- Hepatic triglyceride synthesis increases
- VLDL production increases
- HDL cholesterol decreases
These changes create a highly atherogenic lipid profile that promotes vascular injury and plaque formation.
Cardiovascular Consequences
- The lipid abnormalities associated with obesity and metabolic syndrome significantly accelerate the development of atherosclerosis.
- Excess LDL cholesterol and triglyceride-rich lipoproteins accumulate within arterial walls, initiating inflammatory processes that lead to plaque formation.
As a result, individuals with obesity and metabolic syndrome are at increased risk of:
- Coronary artery disease
- Myocardial infarction
- Stroke
- Peripheral arterial disease
- Heart failure
Cardiovascular disease remains the leading cause of death among patients with metabolic syndrome.
Lipid Profile and Non-Alcoholic Fatty Liver Disease (NAFLD)
- Obesity and metabolic syndrome are strongly associated with non-alcoholic fatty liver disease (NAFLD).
- Excess free fatty acids delivered to the liver promote triglyceride accumulation within hepatocytes, resulting in hepatic steatosis.
Many patients with NAFLD exhibit:
- Elevated triglycerides
- Increased VLDL levels
- Reduced HDL cholesterol
- Insulin resistance
The coexistence of NAFLD and dyslipidemia further increases cardiovascular risk.
Obesity, Inflammation, and Lipid Abnormalities
Adipose tissue in obese individuals produces numerous inflammatory mediators, including:
- Tumor necrosis factor-alpha (TNF-α)
- Interleukin-6 (IL-6)
- C-reactive protein (CRP)
These inflammatory molecules contribute to:
- Endothelial dysfunction
- Oxidative stress
- Insulin resistance
- Altered lipid metabolism
As a result, obesity-associated dyslipidemia is increasingly recognized as both a metabolic and inflammatory disorder.
Importance of Lipid Profile Assessment
Lipid profile evaluation is an important component of the clinical assessment of obese individuals and patients with metabolic syndrome.
Assessment of lipid abnormalities helps:
- Identify cardiovascular risk
- Detect atherogenic dyslipidemia
- Monitor metabolic health
- Evaluate treatment response
- Guide preventive strategies
Lipid Profile in Liver Disease
- The liver is the central organ responsible for lipid metabolism and plays a crucial role in the synthesis, transport, storage, and degradation of lipids and lipoproteins.
- Nearly every component measured in a lipid profile is directly or indirectly influenced by hepatic function.
- Consequently, liver diseases often produce significant alterations in blood lipid concentrations.

The liver performs several essential functions related to lipid metabolism, including:
- Synthesis of cholesterol
- Production of triglycerides
- Formation of lipoproteins
- Conversion of cholesterol into bile acids
- Metabolism of fatty acids
- Regulation of lipid transport
Any impairment in these processes can lead to abnormalities in the lipid profile.
Non-Alcoholic Fatty Liver Disease (NAFLD)
- Non-alcoholic fatty liver disease is one of the most common liver disorders worldwide and is closely associated with obesity, insulin resistance, type 2 diabetes mellitus, and metabolic syndrome.
- In NAFLD, excessive triglycerides accumulate within hepatocytes, resulting in hepatic steatosis.
Patients frequently exhibit a characteristic lipid profile that includes:
- Elevated triglycerides
- Increased VLDL cholesterol
- Reduced HDL cholesterol
- Increased small dense LDL particles
These lipid abnormalities contribute to both liver injury and cardiovascular disease.
Alcoholic Liver Disease
- Chronic alcohol consumption alters lipid metabolism through multiple mechanisms.
- Alcohol increases hepatic triglyceride synthesis and reduces fatty acid oxidation, leading to fat accumulation within liver cells.
As a result, many patients develop:
- Elevated triglycerides
- Increased VLDL production
- Fatty liver changes
Persistent alcohol-related dyslipidemia may increase the risk of pancreatitis and cardiovascular complications.
Cirrhosis
Cirrhosis represents the advanced stage of chronic liver disease characterized by extensive fibrosis and loss of functional liver tissue.
As liver function declines:
- Cholesterol synthesis decreases
- Lipoprotein production decreases
- Triglyceride metabolism becomes impaired
Consequently, patients with advanced cirrhosis may demonstrate reduced levels of:
- Total cholesterol
- LDL cholesterol
- HDL cholesterol
Paradoxically, low cholesterol concentrations in severe liver disease often reflect impaired hepatic synthetic function rather than improved cardiovascular health.
Cholestatic Liver Disease
In cholestatic disorders, bile flow from the liver is impaired.
Because bile is essential for cholesterol elimination, cholestasis can lead to:
- Elevated total cholesterol
- Increased phospholipids
- Accumulation of abnormal lipoproteins
These changes may significantly alter the lipid profile and aid in the diagnosis of hepatobiliary disease.
Lipid Profile in Kidney Disease
- Kidney disease is frequently associated with significant disturbances in lipid metabolism.
- Dyslipidemia is particularly common in patients with chronic kidney disease (CKD), nephrotic syndrome, and end-stage renal disease.
- The kidneys contribute indirectly to lipid metabolism through their influence on hormone regulation, protein metabolism, and enzyme activity.
- When renal function declines, characteristic lipid abnormalities often develop.
- Dyslipidemia in Chronic Kidney Disease.
Patients with CKD commonly exhibit a distinctive pattern of lipid abnormalities characterized by:
- Elevated triglycerides
- Increased VLDL cholesterol
- Reduced HDL cholesterol
- Normal or mildly elevated LDL cholesterol
These changes result from impaired clearance of triglyceride-rich lipoproteins and altered lipoprotein metabolism.
Mechanisms of Dyslipidemia in CKD
Several factors contribute to lipid abnormalities in chronic kidney disease:
- Reduced lipoprotein lipase activity
- Impaired triglyceride metabolism
- Chronic inflammation
- Oxidative stress
- Insulin resistance
Together, these abnormalities promote atherosclerosis and cardiovascular disease.
Nephrotic Syndrome
Nephrotic syndrome is characterized by:
- Massive proteinuria
- Hypoalbuminemia
- Generalized edema
- Hyperlipidemia
Loss of proteins through urine stimulates the liver to increase protein synthesis. Simultaneously, hepatic production of lipoproteins also increases.
As a result, patients frequently develop:
- Markedly elevated total cholesterol
- Increased LDL cholesterol
- Elevated triglycerides
- Increased VLDL cholesterol
Hyperlipidemia in nephrotic syndrome can be severe and may persist until the underlying renal disorder is controlled.
End-Stage Renal Disease
Patients with advanced renal failure often exhibit profound lipid abnormalities.
These changes may include:
- Elevated triglycerides
- Reduced HDL cholesterol
- Increased oxidative modification of LDL particles
Such alterations contribute significantly to the high cardiovascular mortality observed among dialysis patients.
Cardiovascular Implications
Cardiovascular disease is the leading cause of death in patients with chronic kidney disease.
Dyslipidemia contributes to:
- Endothelial dysfunction
- Atherosclerosis
- Coronary artery disease
- Stroke
- Peripheral vascular disease
Therefore, lipid profile monitoring is an important component of renal disease management.
Inherited Lipid Disorders
- Inherited lipid disorders are genetic conditions that affect the synthesis, transport, metabolism, or clearance of lipids and lipoproteins.
- These disorders often result in severe dyslipidemia and markedly increased cardiovascular risk.
- Although relatively uncommon, inherited dyslipidemias are clinically important because they frequently present at a young age and may lead to premature cardiovascular disease.
Familial Hypercholesterolemia (FH)
Familial hypercholesterolemia is one of the most common inherited lipid disorders.
It results from mutations affecting:
- LDL receptor genes
- Apolipoprotein B genes
- PCSK9 genes
These mutations impair the removal of LDL cholesterol from circulation, leading to markedly elevated LDL concentrations.
Clinical Features
Patients may develop:
- Tendon xanthomas
- Xanthelasma
- Corneal arcus
- Premature coronary artery disease
Affected individuals often experience cardiovascular events decades earlier than the general population.
Familial Combined Hyperlipidemia
Familial combined hyperlipidemia is among the most common inherited causes of dyslipidemia.
Patients may exhibit:
- Elevated LDL cholesterol
- Elevated triglycerides
- Increased VLDL production
The disorder significantly increases the risk of premature atherosclerosis and coronary artery disease.
Familial Hypertriglyceridemia
- This condition is characterized by excessive triglyceride production or impaired triglyceride clearance.
Affected individuals typically have:
- Markedly elevated triglycerides
- Increased VLDL cholesterol
- Normal or mildly elevated cholesterol
Severe hypertriglyceridemia increases the risk of acute pancreatitis.
Familial Dysbetalipoproteinemia
- This rare disorder results from abnormalities in apolipoprotein E metabolism.
Patients often demonstrate:
- Elevated cholesterol
- Elevated triglycerides
- Increased remnant lipoproteins
The disorder is strongly associated with premature atherosclerosis.
Clinical Manifestations of Inherited Dyslipidemias
Common clinical signs include:
- Xanthomas
- Xanthelasma
- Corneal arcus
- Premature cardiovascular disease
- Early myocardial infarction
- Peripheral vascular disease
The severity of manifestations depends on the specific genetic defect and degree of lipid abnormality.
Importance of Early Detection
Early recognition of inherited lipid disorders is essential because affected individuals may appear healthy despite significantly increased cardiovascular risk.
Identification allows:
- Risk assessment
- Family screening
- Early lifestyle intervention
- Appropriate medical therapy
- Prevention of cardiovascular complications