Introduction
- Mineral metabolism refers to the absorption, transport, storage, utilization, and excretion of minerals in the body.
- Minerals are essential inorganic nutrients required for normal growth, development, and maintenance of health.
- They play important roles in bone formation, muscle contraction, nerve transmission, enzyme activity, and fluid balance.
- Minerals are classified into major minerals (calcium, phosphorus, magnesium, sodium, potassium) and trace minerals (iron, zinc, copper, iodine, selenium).
- The body maintains mineral balance through coordinated actions of the intestine, kidneys, bones, and various hormones.
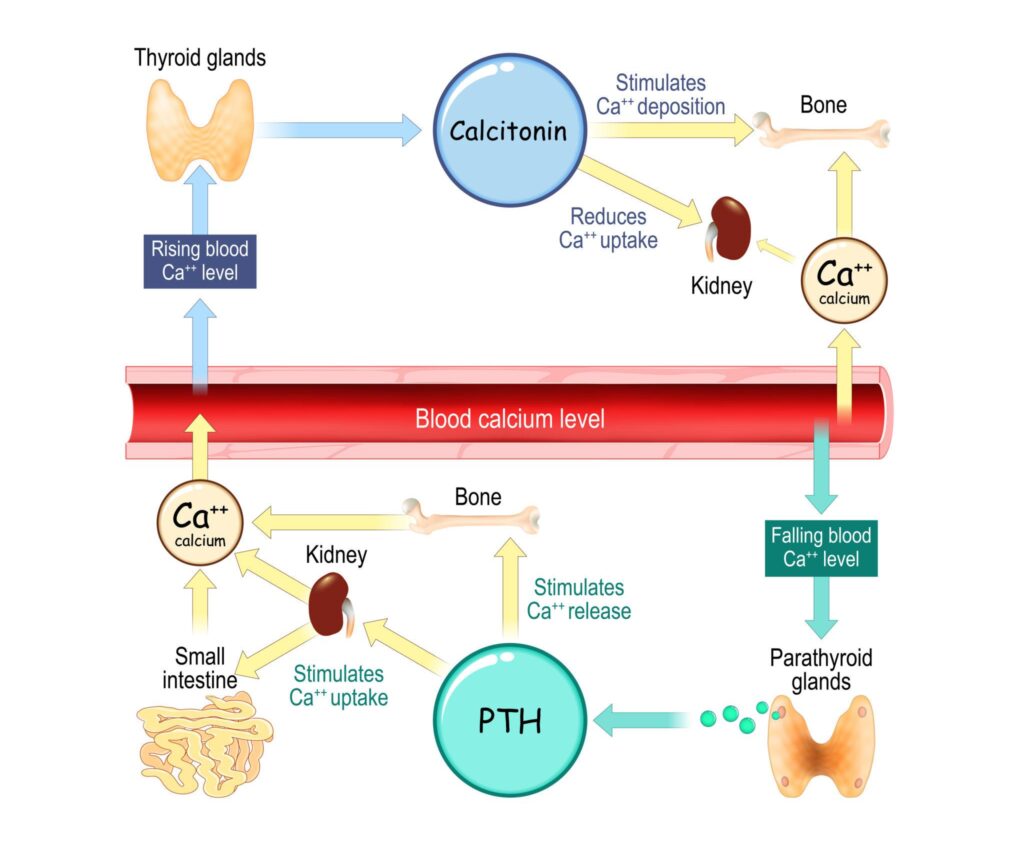
- Key hormones involved in mineral regulation include parathyroid hormone (PTH), vitamin D, calcitonin, and hepcidin.
- Abnormal mineral metabolism can lead to disorders such as osteoporosis, anemia, rickets, goiter, and electrolyte imbalances.
- Understanding mineral metabolism is important for diagnosing and managing many metabolic and endocrine diseases.
General Functions of Minerals
- Formation of Bones and Teeth
- Minerals such as calcium, phosphorus, and magnesium provide strength and structure to bones and teeth.
- Enzyme Activation
- Many minerals act as cofactors and are required for the activity of various enzymes involved in metabolism.
- Nerve Impulse Transmission
- Sodium, potassium, calcium, and magnesium help in the generation and transmission of nerve impulses.
- Muscle Contraction
- Calcium, magnesium, potassium, and sodium are essential for normal muscle contraction and relaxation.
- Maintenance of Fluid and Electrolyte Balance
- Sodium, potassium, and chloride regulate the distribution of water between body compartments.
- Acid-Base Balance
- Minerals help maintain the normal pH of body fluids through various buffer systems.
- Oxygen Transport
- Iron is a key component of hemoglobin and is essential for oxygen transport in the blood.
- Hormone and Vitamin Function
- Iodine is required for thyroid hormone synthesis, while several minerals assist in hormone action and vitamin metabolism.
- Energy Production
- Phosphorus is a component of ATP, the primary energy currency of the cell.
- Cell Growth and Immune Function
- Trace elements such as zinc, selenium, and copper are important for cell division, wound healing, antioxidant defense, and immune responses.
Classification of Minerals
Minerals are classified based on the amount required by the body into Major Minerals (Macrominerals) and Trace Minerals (Microminerals).
| Category | Daily Requirement | Minerals |
|---|---|---|
| Major Minerals (Macrominerals) | More than 100 mg/day | Calcium (Ca), Phosphorus (P), Magnesium (Mg), Sodium (Na), Potassium (K), Chloride (Cl), Sulfur (S) |
| Trace Minerals (Microminerals) | Less than 100 mg/day | Iron (Fe), Zinc (Zn), Copper (Cu), Iodine (I), Selenium (Se), Manganese (Mn), Chromium (Cr), Molybdenum (Mo), Fluoride (F), Cobalt (Co) |
1. Major Minerals (Macrominerals)
These minerals are required in relatively large amounts and are essential for structural and physiological functions.
Examples and Functions:
- Calcium – Bone and teeth formation, muscle contraction.
- Phosphorus – ATP production, bone mineralization.
- Magnesium – Enzyme activation, neuromuscular function.
- Sodium – Fluid balance and nerve conduction.
- Potassium – Muscle function and maintenance of membrane potential.
- Chloride – Acid-base balance and gastric acid formation.
- Sulfur – Component of amino acids and proteins.
2. Trace Minerals (Microminerals)
These minerals are required in small quantities but are vital for numerous metabolic processes.
Examples and Functions:
- Iron – Oxygen transport and hemoglobin synthesis.
- Zinc – Enzyme activity, immunity, and wound healing.
- Copper – Iron metabolism and antioxidant defense.
- Iodine – Thyroid hormone synthesis.
- Selenium – Antioxidant protection.
- Manganese – Bone formation and enzyme activation.
- Chromium – Glucose metabolism.
- Molybdenum – Cofactor for several enzymes.
- Fluoride – Strengthens teeth and bones.
- Cobalt – Component of Vitamin B₁₂.
Macrominerals
Calcium
Introduction
- Calcium is the most abundant mineral in the human body and is essential for normal growth, development, and maintenance of physiological functions.
- An adult human body contains approximately 1000–1200 g of calcium, with about 99% present in bones and teeth as hydroxyapatite crystals and the remaining 1% found in blood, extracellular fluid, and soft tissues.
- Calcium plays a crucial role in skeletal integrity, neuromuscular activity, blood coagulation, and intracellular signaling.
Biochemical Functions of Calcium
- Formation and maintenance of bones and teeth.
- Muscle contraction, including cardiac muscle function.
- Transmission of nerve impulses.
- Blood coagulation (acts as Factor IV in the clotting cascade).
- Activation of various enzymes.
- Regulation of hormone and neurotransmitter release.
- Maintenance of cell membrane permeability.
- Intracellular signaling through calcium-dependent pathways.
- Regulation of heartbeat and cardiac rhythm.
Dietary Requirement of Calcium
| Age Group | Requirement (mg/day) |
|---|---|
| Infants (0–12 months) | 200–260 |
| Children (1–8 years) | 700–1000 |
| Adolescents (9–18 years) | 1300 |
| Adults (19–50 years) | 1000 |
| Adults (>50 years) | 1200 |
| Pregnant and Lactating Women | 1000–1300 |
Sources of Calcium
Calcium is widely distributed in both animal and plant foods.
| Food Source | Calcium Content |
|---|---|
| Milk and Dairy Products | Excellent source |
| Cheese | Excellent source |
| Yogurt | Excellent source |
| Ragi (Finger Millet) | Rich source |
| Sesame Seeds | Rich source |
| Almonds | Good source |
| Soybeans and Tofu | Good source |
| Green Leafy Vegetables | Moderate source |
| Fortified Cereals and Juices | Variable source |
Absorption of Calcium
Calcium is absorbed mainly in the duodenum and proximal jejunum.
Two mechanisms are involved:
1. Active Transport
- Predominantly occurs when dietary calcium intake is low.
- Vitamin D dependent.
- Most effective in the duodenum.
2. Passive Diffusion
- Occurs throughout the small intestine.
- Independent of Vitamin D.
- Becomes significant when calcium intake is high.
Normally, 20–40% of dietary calcium is absorbed, depending on age, dietary composition, and vitamin D status.
Factors Promoting Calcium Absorption
| Factor | Mechanism |
|---|---|
| Vitamin D (Calcitriol) | Increases calcium transport proteins |
| Acidic Gastric pH | Keeps calcium soluble |
| Lactose | Enhances intestinal absorption |
| Adequate Dietary Protein | Improves absorption |
| Growth Hormone | Increases calcium retention |
| Pregnancy and Lactation | Increased physiological demand |
| Certain Amino Acids | Improve calcium solubility |
Factors Inhibiting Calcium Absorption
| Factor | Mechanism |
|---|---|
| Phytates (cereals, grains) | Form insoluble calcium complexes |
| Oxalates (spinach, beetroot) | Reduce calcium bioavailability |
| Excess Dietary Fiber | Decreases absorption |
| Vitamin D Deficiency | Impairs active transport |
| Alkaline Intestinal pH | Reduces calcium solubility |
| Malabsorption Syndromes | Decrease intestinal uptake |
| Excess Phosphate Intake | Forms insoluble salts |
Disease States Associated with Calcium Metabolism
1. Hypocalcemia
Hypocalcemia refers to a decrease in serum calcium concentration below the normal range.
Causes
- Vitamin D deficiency
- Hypoparathyroidism
- Chronic kidney disease
- Acute pancreatitis
- Malabsorption disorders
Clinical Features
- Muscle cramps
- Tetany
- Paresthesia
- Seizures
- Positive Chvostek sign
- Positive Trousseau sign
2. Hypercalcemia
Hypercalcemia is characterized by elevated serum calcium levels.
Causes
- Primary hyperparathyroidism
- Malignancy
- Vitamin D intoxication
- Prolonged immobilization
Clinical Features
- Kidney stones
- Bone pain
- Constipation
- Polyuria
- Fatigue
- Mental confusion
3. Rickets
- Occurs in children due to vitamin D and calcium deficiency.
- Characterized by defective mineralization of growing bones.
Features
- Bowed legs
- Delayed dentition
- Skeletal deformities
- Growth retardation
4. Osteomalacia
- Adult counterpart of rickets.
- Characterized by defective mineralization of bone matrix.
Features
- Bone pain
- Muscle weakness
- Increased fracture risk
5. Osteoporosis
- Progressive reduction in bone mass and density.
- Common in postmenopausal women and elderly individuals.
Risk Factors
- Aging
- Estrogen deficiency
- Low calcium intake
- Physical inactivity
Features
- Fragility fractures
- Vertebral compression
- Loss of height
| Disorder | Serum Calcium | Major Cause |
|---|---|---|
| Hypocalcemia | ↓ | Vitamin D deficiency, hypoparathyroidism |
| Hypercalcemia | ↑ | Hyperparathyroidism, malignancy |
| Rickets | Usually ↓ | Vitamin D deficiency in children |
| Osteomalacia | Normal or ↓ | Defective bone mineralization |
| Osteoporosis | Usually Normal | Reduced bone mass |
Phosphorus
Introduction
- Phosphorus is the second most abundant mineral in the human body after calcium.
- It is present mainly in the form of phosphate and plays a vital role in skeletal structure, energy metabolism, cell signaling, and acid-base balance.
- An adult human body contains approximately 700 g of phosphorus, with about 85% present in bones and teeth, while the remaining is distributed in soft tissues and extracellular fluids.
Biochemical Functions of Phosphorus
- Formation and mineralization of bones and teeth.
- Essential component of ATP, ADP, and AMP involved in energy transfer.
- Constituent of nucleic acids (DNA and RNA).
- Component of phospholipids in cell membranes.
- Maintains acid-base balance through the phosphate buffer system.
- Participates in phosphorylation reactions and cell signaling.
- Required for normal muscle and nerve function.
- Involved in carbohydrate, lipid, and protein metabolism.
Dietary Requirement of Phosphorus
| Age Group | Requirement (mg/day) |
|---|---|
| Infants (0–12 months) | 100–275 |
| Children (1–8 years) | 460–500 |
| Adolescents (9–18 years) | 1250 |
| Adults (19 years and above) | 700 |
| Pregnant and Lactating Women | 700–1250 |
Sources of Phosphorus
Phosphorus is widely distributed in both animal and plant foods.
| Food Source | Phosphorus Content |
|---|---|
| Milk and Dairy Products | Rich source |
| Meat and Poultry | Rich source |
| Fish and Seafood | Rich source |
| Eggs | Good source |
| Nuts and Seeds | Good source |
| Legumes and Pulses | Good source |
| Whole Grains | Moderate source |
| Processed Foods and Soft Drinks | High phosphate additives |
Absorption of Phosphorus
Phosphate is absorbed mainly in the duodenum and jejunum.
Two mechanisms are involved:
1. Active Transport
- Vitamin D dependent.
- Occurs when phosphate intake is low.
- Facilitated by sodium-phosphate cotransporters.
2. Passive Diffusion
- Occurs when dietary phosphate intake is high.
- Independent of vitamin D.
Normally, 60–80% of dietary phosphorus is absorbed in healthy individuals.
Factors Promoting Phosphorus Absorption
| Factor | Mechanism |
|---|---|
| Vitamin D (Calcitriol) | Increases intestinal phosphate transport |
| Adequate Dietary Intake | Ensures sufficient absorption |
| Acidic Intestinal Environment | Improves phosphate solubility |
| Growth and Pregnancy | Increase phosphate utilization and absorption |
Factors Inhibiting Phosphorus Absorption
| Factor | Mechanism |
|---|---|
| Excess Calcium Intake | Forms insoluble calcium phosphate |
| Aluminum-containing Antacids | Bind phosphate in the intestine |
| Magnesium-containing Antacids | Reduce phosphate absorption |
| Vitamin D Deficiency | Decreases active transport |
| Malabsorption Syndromes | Reduce intestinal uptake |
| Chronic Diarrhea | Decreases absorption time |
Regulation of Phosphate Homeostasis
Phosphate balance is maintained by the coordinated action of:
- Parathyroid Hormone (PTH)
- Vitamin D (Calcitriol)
- Fibroblast Growth Factor-23 (FGF23)
| Hormone | Effect on Serum Phosphate |
|---|---|
| PTH | Decreases phosphate by increasing renal excretion |
| Vitamin D | Increases intestinal phosphate absorption |
| FGF23 | Decreases phosphate by reducing renal reabsorption |
Disease States Associated with Phosphorus Metabolism
1. Hypophosphatemia
Hypophosphatemia refers to a decrease in serum phosphate levels below the normal range.
Causes
- Vitamin D deficiency
- Hyperparathyroidism
- Malnutrition
- Chronic alcoholism
- Refeeding syndrome
Clinical Features
- Muscle weakness
- Bone pain
- Osteomalacia
- Rickets
- Respiratory failure in severe cases
2. Hyperphosphatemia
Hyperphosphatemia is characterized by elevated serum phosphate levels.
Causes
- Chronic kidney disease
- Hypoparathyroidism
- Excess phosphate intake
- Tumor lysis syndrome
Clinical Features
- Soft tissue calcification
- Pruritus
- Secondary hypocalcemia
- Muscle cramps
3. Rickets
- Occurs in children due to defective mineralization of growing bones.
- Often associated with calcium and phosphate deficiency.
Features
- Bowed legs
- Delayed growth
- Skeletal deformities
4. Osteomalacia
- Characterized by inadequate mineralization of bone matrix in adults.
- Commonly associated with phosphate and vitamin D deficiency.
Features
- Bone pain
- Muscle weakness
- Increased fracture risk
| Disorder | Serum Phosphate | Major Cause |
|---|---|---|
| Hypophosphatemia | ↓ | Vitamin D deficiency, hyperparathyroidism |
| Hyperphosphatemia | ↑ | Chronic kidney disease, hypoparathyroidism |
| Rickets | ↓ or Normal | Defective bone mineralization in children |
| Osteomalacia | ↓ or Normal | Defective bone mineralization in adults |
Normal Serum Phosphate Levels
Table 8. Reference Range of Serum Phosphate
| Age Group | Serum Phosphate (mg/dL) |
|---|---|
| Children | 4.0–7.0 |
| Adults | 2.5–4.5 |
Magnesium
Introduction
- Magnesium is the fourth most abundant cation in the human body and the second most abundant intracellular cation after potassium.
- An adult human body contains approximately 25 g of magnesium, with about 60% present in bones, 20% in skeletal muscles, and the remainder in soft tissues and body fluids.
- Magnesium is essential for numerous biochemical reactions and serves as a cofactor for more than 300 enzymes involved in energy production, protein synthesis, and nucleic acid metabolism.
Biochemical Functions of Magnesium
| Function | Role |
|---|---|
| Enzyme Activation | Cofactor for numerous enzymes |
| Energy Metabolism | Required for ATP-dependent reactions |
| Protein Synthesis | Facilitates ribosomal activity |
| Nucleic Acid Synthesis | Essential for DNA and RNA synthesis |
| Neuromuscular Function | Regulates nerve and muscle activity |
| Cardiac Function | Maintains normal heart rhythm |
| Bone Health | Contributes to bone mineralization |
Dietary Requirement of Magnesium
| Age Group | Requirement (mg/day) |
|---|---|
| Infants (0–12 months) | 30–75 |
| Children (1–8 years) | 80–130 |
| Adolescents (9–18 years) | 240–410 |
| Adult Men | 400–420 |
| Adult Women | 310–320 |
| Pregnant Women | 350–400 |
| Lactating Women | 310–360 |
Sources of Magnesium
Magnesium is widely distributed in plant and animal foods.
| Food Source | Magnesium Content |
|---|---|
| Green Leafy Vegetables | Rich source |
| Nuts (Almonds, Cashews) | Rich source |
| Seeds (Pumpkin, Sesame) | Rich source |
| Whole Grains | Good source |
| Legumes and Pulses | Good source |
| Soy Products | Good source |
| Dark Chocolate | Good source |
| Bananas | Moderate source |
| Milk and Dairy Products | Moderate source |
Absorption of Magnesium
Magnesium is absorbed mainly in the small intestine, particularly the jejunum and ileum.
Two mechanisms are involved:
1. Passive Diffusion
- Major mechanism of absorption.
- Occurs when dietary magnesium intake is high.
2. Active Transport
- Operates when magnesium intake is low.
- Regulated according to body requirements.
Normally, 30–50% of dietary magnesium is absorbed.
Factors Promoting Magnesium Absorption
| Factor | Mechanism |
|---|---|
| Vitamin D | Improves intestinal absorption |
| Adequate Dietary Protein | Enhances uptake |
| Growth and Pregnancy | Increase magnesium utilization |
| Increased Physiological Demand | Stimulates absorption |
Factors Inhibiting Magnesium Absorption
| Factor | Mechanism |
|---|---|
| Excess Calcium Intake | Competes with magnesium absorption |
| Phytates | Form insoluble complexes |
| Excess Dietary Fiber | Decreases absorption |
| Chronic Diarrhea | Reduces intestinal uptake |
| Malabsorption Syndromes | Impair absorption |
| Alcoholism | Decreases intestinal absorption |
Magnesium Homeostasis
Magnesium balance is maintained by:
- Intestinal absorption
- Bone storage
- Renal excretion
The kidneys play a major role in regulating serum magnesium levels by adjusting tubular reabsorption according to body needs.
Normal Serum Magnesium Levels
Table 6. Reference Range of Serum Magnesium
| Parameter | Reference Range |
|---|---|
| Serum Magnesium | 1.7–2.4 mg/dL |
| Ionized Magnesium | 0.45–0.60 mmol/L |
Disease States Associated with Magnesium Metabolism
1. Hypomagnesemia
Hypomagnesemia refers to a decrease in serum magnesium concentration below normal levels.
Causes
- Chronic alcoholism
- Malnutrition
- Chronic diarrhea
- Malabsorption syndromes
- Diuretic therapy
- Uncontrolled diabetes mellitus
Clinical Features
- Muscle weakness
- Tremors
- Tetany
- Muscle cramps
- Seizures
- Cardiac arrhythmias
- Increased neuromuscular excitability
2. Hypermagnesemia
Hypermagnesemia is characterized by elevated serum magnesium levels.
Causes
- Chronic kidney disease
- Renal failure
- Excess magnesium-containing antacids or laxatives
- Excessive magnesium supplementation
Clinical Features
- Nausea and vomiting
- Muscle weakness
- Hypotension
- Bradycardia
- Respiratory depression
- Cardiac arrest in severe cases
3. Magnesium Deficiency
Long-term magnesium deficiency may contribute to:
- Osteoporosis
- Hypertension
- Cardiovascular disease
- Insulin resistance
- Migraine headaches
| Disorder | Serum Magnesium | Major Cause |
|---|---|---|
| Hypomagnesemia | ↓ | Alcoholism, malabsorption, diarrhea |
| Hypermagnesemia | ↑ | Renal failure, excess magnesium intake |
| Magnesium Deficiency | ↓ | Poor dietary intake, chronic illness |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Serum Magnesium | Initial screening test |
| Ionized Magnesium | Biologically active form |
| Urinary Magnesium | Assesses renal magnesium handling |
| Serum Calcium and Potassium | Often abnormal in magnesium disorders |
| Renal Function Tests | Evaluate underlying kidney disease |
Sodium
Introduction
- Sodium is the principal cation of the extracellular fluid (ECF) and is the most important electrolyte involved in maintaining fluid balance, osmotic pressure, acid-base balance, and neuromuscular function.
- An adult human body contains approximately 90–100 g of sodium, with nearly 50% present in extracellular fluids, 40% in bones, and the remainder within cells.
- Sodium homeostasis is primarily regulated by the kidneys under the influence of hormones such as aldosterone, antidiuretic hormone (ADH), and atrial natriuretic peptide (ANP).
Biochemical Functions of Sodium
| Function | Role |
|---|---|
| Fluid Balance | Maintains extracellular fluid volume |
| Osmotic Pressure | Regulates water distribution |
| Nerve Function | Generation and transmission of nerve impulses |
| Muscle Function | Required for muscle contraction |
| Acid-Base Balance | Helps maintain normal blood pH |
| Nutrient Absorption | Facilitates absorption of glucose and amino acids |
| Blood Pressure Regulation | Influences vascular volume and pressure |
Dietary Requirement of Sodium
| Age Group | Requirement (mg/day) |
|---|---|
| Children | 1000–1500 |
| Adults | 1500–2300 |
| Pregnant Women | 1500–2300 |
| Lactating Women | 1500–2300 |
WHO Recommendation: Sodium intake should be less than 2000 mg/day (equivalent to approximately 5 g of salt per day).
Sources of Sodium
| Food Source | Sodium Content |
|---|---|
| Table Salt (NaCl) | Excellent source |
| Pickles | Rich source |
| Processed Foods | Rich source |
| Canned Foods | Rich source |
| Bakery Products | Moderate source |
| Cheese | Moderate source |
| Meat and Fish | Moderate source |
| Milk | Small amount |
| Vegetables | Small amount |
Absorption of Sodium
Sodium is absorbed efficiently throughout the small intestine and colon.
Mechanism of Absorption
1. Active Transport
- Sodium is actively transported across intestinal epithelial cells.
- Mediated by the Na⁺/K⁺ ATPase pump.
2. Co-transport Mechanism
- Sodium absorption is coupled with glucose and amino acid absorption.
Normally, more than 95% of dietary sodium is absorbed.
Factors Promoting Sodium Absorption
| Factor | Mechanism |
|---|---|
| Glucose | Sodium-glucose co-transport |
| Amino Acids | Sodium-amino acid co-transport |
| Aldosterone | Increases intestinal and renal sodium reabsorption |
| Adequate Hydration | Supports normal absorption |
| Oral Rehydration Solution (ORS) | Enhances sodium uptake through co-transport |
Factors Inhibiting Sodium Absorption
| Factor | Mechanism |
|---|---|
| Chronic Diarrhea | Increased sodium loss |
| Intestinal Malabsorption | Reduced absorption |
| Severe Vomiting | Excess sodium loss |
| Adrenal Insufficiency | Decreased sodium retention |
| Certain Diuretics | Increased renal sodium excretion |
Regulation of Sodium Homeostasis
Sodium balance is maintained mainly by the kidneys.
Important Hormones
1. Aldosterone
- Increases sodium reabsorption in renal tubules.
- Promotes water retention.
2. Antidiuretic Hormone (ADH)
- Regulates water balance and indirectly influences sodium concentration.
3. Atrial Natriuretic Peptide (ANP)
- Increases sodium excretion by the kidneys.
- Lowers blood volume and blood pressure.
Normal Serum Sodium Levels
| Parameter | Reference Range |
|---|---|
| Serum Sodium | 135–145 mEq/L |
Disease States Associated with Sodium Metabolism
1. Hyponatremia
Hyponatremia refers to serum sodium concentration below 135 mEq/L.
Causes
- Excessive sweating
- Prolonged vomiting
- Chronic diarrhea
- Renal disease
- Syndrome of Inappropriate ADH Secretion (SIADH)
- Heart failure
Clinical Features
- Headache
- Nausea
- Muscle cramps
- Confusion
- Seizures
- Coma in severe cases
2. Hypernatremia
Hypernatremia refers to serum sodium concentration above 145 mEq/L.
Causes
- Dehydration
- Diabetes insipidus
- Excessive sodium intake
- Severe water loss
Clinical Features
- Intense thirst
- Dry mucous membranes
- Irritability
- Muscle twitching
- Confusion
- Seizures
3. Edema
Excess sodium retention can lead to fluid accumulation in tissues.
Causes
- Congestive heart failure
- Nephrotic syndrome
- Liver cirrhosis
- Renal disease
Features
- Swelling of feet and ankles
- Weight gain
- Fluid retention
4. Hypertension
Excess dietary sodium intake is associated with elevated blood pressure and increased cardiovascular risk.
Risk Factors
- High salt consumption
- Obesity
- Kidney disease
- Genetic predisposition
| Disorder | Serum Sodium | Major Cause |
|---|---|---|
| Hyponatremia | ↓ | Diarrhea, SIADH, renal disease |
| Hypernatremia | ↑ | Dehydration, diabetes insipidus |
| Edema | Usually Normal or ↑ Total Body Sodium | Heart, liver, or kidney disease |
| Hypertension | Variable | Excess sodium intake |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Serum Sodium | Primary assessment of sodium status |
| Urinary Sodium | Evaluates renal sodium handling |
| Serum Osmolality | Assesses water balance |
| Renal Function Tests | Detect kidney-related abnormalities |
| Plasma ADH | Evaluation of sodium-water disorders |
Potassium
Introduction
- Potassium is the principal intracellular cation and one of the most important electrolytes in the human body.
- An adult human body contains approximately 120–150 g of potassium, with about 98% located inside cells and only 2% present in the extracellular fluid.
- Potassium is essential for maintaining cellular function, nerve impulse transmission, muscle contraction, acid-base balance, and cardiac activity.
- The kidneys play a major role in regulating potassium homeostasis.
Biochemical Functions of Potassium
- Maintains intracellular osmotic pressure and cell volume.
- Essential for nerve impulse transmission.
- Required for skeletal, smooth, and cardiac muscle contraction.
- Maintains normal cardiac rhythm.
- Participates in acid-base balance.
- Activates various enzymes involved in carbohydrate and protein metabolism.
- Helps regulate blood pressure.
- Essential for normal cellular metabolism and growth.
Dietary Requirement of Potassium
| Age Group | Requirement (mg/day) |
|---|---|
| Children | 2000–3000 |
| Adolescents | 3000–4000 |
| Adult Men | 3400 |
| Adult Women | 2600 |
| Pregnant Women | 2900 |
| Lactating Women | 2800 |
Sources of Potassium
Potassium is abundant in fruits, vegetables, legumes, and whole grains.
| Food Source | Potassium Content |
|---|---|
| Bananas | Rich source |
| Coconut Water | Rich source |
| Potatoes | Rich source |
| Tomatoes | Rich source |
| Spinach | Rich source |
| Avocado | Rich source |
| Legumes and Pulses | Good source |
| Dried Fruits | Good source |
| Milk and Yogurt | Moderate source |
| Nuts and Seeds | Moderate source |
Absorption of Potassium
Potassium is absorbed efficiently from the gastrointestinal tract, mainly in the small intestine.
Mechanism of Absorption
1. Passive Diffusion
- Primary mechanism of absorption.
- Occurs along the concentration gradient.
2. Active Transport
- Contributes to potassium uptake when required.
Normally, 85–95% of dietary potassium is absorbed.
Factors Promoting Potassium Absorption
| Factor | Mechanism |
|---|---|
| Adequate Dietary Intake | Maintains potassium stores |
| Healthy Intestinal Function | Promotes normal absorption |
| Balanced Electrolyte Intake | Supports potassium utilization |
| Physical Growth and Pregnancy | Increase potassium requirements |
Factors Inhibiting Potassium Absorption
| Factor | Mechanism |
|---|---|
| Chronic Diarrhea | Excessive potassium loss |
| Vomiting | Indirect potassium depletion |
| Malabsorption Syndromes | Reduced intestinal uptake |
| Laxative Abuse | Increased gastrointestinal losses |
| Certain Gastrointestinal Disorders | Decreased absorption |
Regulation of Potassium Homeostasis
Potassium balance is regulated primarily by:
- Kidneys
- Aldosterone
- Insulin
- Acid-base status
| Factor | Effect on Potassium |
|---|---|
| Aldosterone | Increases potassium excretion |
| Insulin | Drives potassium into cells |
| Acidosis | Causes potassium to move out of cells |
| Alkalosis | Causes potassium to move into cells |
Normal Serum Potassium Levels
| Parameter | Reference Range |
|---|---|
| Serum Potassium | 3.5–5.0 mEq/L |
Disease States Associated with Potassium Metabolism
1. Hypokalemia
Hypokalemia refers to serum potassium levels below 3.5 mEq/L.
Causes
- Prolonged vomiting
- Chronic diarrhea
- Diuretic therapy
- Hyperaldosteronism
- Poor dietary intake
Clinical Features
- Muscle weakness
- Fatigue
- Muscle cramps
- Constipation
- Paralysis in severe cases
- Cardiac arrhythmias
2. Hyperkalemia
Hyperkalemia refers to serum potassium levels above 5.0 mEq/L.
Causes
- Chronic kidney disease
- Renal failure
- Hypoaldosteronism
- Excess potassium supplementation
- Tissue destruction (burns, trauma)
Clinical Features
- Muscle weakness
- Paresthesia
- Bradycardia
- Cardiac arrhythmias
- Cardiac arrest in severe cases
3. Cardiac Arrhythmias
Abnormal potassium levels significantly affect cardiac conduction and may produce life-threatening arrhythmias.
Effects
- Hypokalemia → Tachyarrhythmias
- Hyperkalemia → Conduction defects and cardiac arrest
| Disorder | Serum Potassium | Major Cause |
|---|---|---|
| Hypokalemia | ↓ | Diarrhea, vomiting, diuretics |
| Hyperkalemia | ↑ | Renal failure, hypoaldosteronism |
| Cardiac Arrhythmias | Variable | Abnormal potassium balance |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Serum Potassium | Primary assessment of potassium status |
| Urinary Potassium | Evaluation of renal potassium handling |
| Blood Gas Analysis | Assessment of acid-base disorders |
| ECG | Detects cardiac effects of potassium abnormalities |
| Renal Function Tests | Evaluate kidney-related causes |
Chloride (Chlorine)
Introduction
- Chloride is the principal extracellular anion and is usually present in the body in association with sodium as sodium chloride (NaCl).
- An adult human body contains approximately 95–105 g of chloride, most of which is found in the extracellular fluid.
- Chloride plays a vital role in maintaining osmotic pressure, fluid balance, acid-base equilibrium, and gastric acid formation.
- It is an essential electrolyte required for normal cellular and physiological functions.
Biochemical Functions of Chloride
- Maintains osmotic pressure and water balance.
- Helps regulate acid-base balance.
- Essential component of hydrochloric acid (HCl) in gastric juice.
- Participates in the transport of carbon dioxide in blood.
- Maintains electrical neutrality in body fluids.
- Assists in digestion and nutrient absorption.
- Contributes to nerve impulse transmission.
Dietary Requirement of Chloride
| Age Group | Requirement (mg/day) |
|---|---|
| Children | 1500–1900 |
| Adolescents | 2300 |
| Adults | 2300 |
| Pregnant Women | 2300 |
| Lactating Women | 2300 |
Sources of Chloride
Chloride is widely available in foods, primarily as sodium chloride (common salt).
| Food Source | Chloride Content |
|---|---|
| Table Salt (NaCl) | Excellent source |
| Processed Foods | Rich source |
| Pickles | Rich source |
| Cheese | Good source |
| Meat and Fish | Good source |
| Milk | Moderate source |
| Tomatoes | Moderate source |
| Lettuce and Celery | Moderate source |
| Seaweed | Rich source |
Absorption of Chloride
Chloride is absorbed efficiently from the gastrointestinal tract, mainly in the small intestine.
Mechanism of Absorption
1. Passive Absorption
- Chloride follows sodium absorption through electrochemical gradients.
2. Active Transport
- Occurs through chloride channels and chloride-bicarbonate exchangers.
Normally, more than 95% of dietary chloride is absorbed.
Factors Promoting Chloride Absorption
| Factor | Mechanism |
|---|---|
| Sodium Absorption | Chloride follows sodium movement |
| Adequate Dietary Salt Intake | Provides chloride ions |
| Normal Intestinal Function | Ensures efficient absorption |
| Proper Hydration | Supports electrolyte balance |
Factors Inhibiting Chloride Absorption
| Factor | Mechanism |
|---|---|
| Chronic Diarrhea | Increased chloride loss |
| Prolonged Vomiting | Loss of gastric chloride |
| Malabsorption Syndromes | Reduced intestinal uptake |
| Excessive Sweating | Increased chloride loss |
| Certain Diuretics | Increased renal chloride excretion |
Chloride Homeostasis
Chloride balance is maintained primarily by:
- Kidneys
- Gastrointestinal tract
- Sweat glands
The kidneys regulate chloride levels by controlling its reabsorption and excretion.
Normal Serum Chloride Levels
| Parameter | Reference Range |
|---|---|
| Serum Chloride | 98–106 mEq/L |
Disease States Associated with Chloride Metabolism
1. Hypochloremia
Hypochloremia refers to serum chloride levels below 98 mEq/L.
Causes
- Prolonged vomiting
- Chronic diarrhea
- Excessive sweating
- Diuretic therapy
- Metabolic alkalosis
Clinical Features
- Muscle weakness
- Dehydration
- Fatigue
- Muscle cramps
- Shallow breathing
2. Hyperchloremia
Hyperchloremia refers to serum chloride levels above 106 mEq/L.
Causes
- Dehydration
- Renal disease
- Excessive saline administration
- Metabolic acidosis
Clinical Features
- Thirst
- Weakness
- Elevated blood pressure
- Rapid breathing
- Confusion
3. Metabolic Alkalosis
- Often associated with chloride depletion due to prolonged vomiting.
- Reduced chloride impairs bicarbonate excretion, leading to alkalosis.
4. Metabolic Acidosis
- Hyperchloremic metabolic acidosis occurs when chloride levels increase excessively relative to bicarbonate.
Causes
- Severe diarrhea
- Renal tubular acidosis
- Excessive saline infusion
| Disorder | Serum Chloride | Major Cause |
|---|---|---|
| Hypochloremia | ↓ | Vomiting, diuretics, diarrhea |
| Hyperchloremia | ↑ | Dehydration, metabolic acidosis |
| Metabolic Alkalosis | ↓ | Gastric acid loss |
| Hyperchloremic Acidosis | ↑ | Diarrhea, renal tubular acidosis |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Serum Chloride | Primary assessment of chloride status |
| Electrolyte Panel | Evaluates sodium, potassium, and chloride balance |
| Arterial Blood Gas (ABG) | Assessment of acid-base disorders |
| Serum Bicarbonate | Helps identify metabolic acidosis or alkalosis |
| Renal Function Tests | Evaluation of kidney-related causes |
Sulfur
Introduction
- Sulfur is an essential mineral that is present in all living cells and is a major component of several amino acids, proteins, vitamins, and enzymes.
- Unlike other minerals, sulfur is not usually required as a separate dietary nutrient because it is obtained primarily from sulfur-containing amino acids such as methionine and cysteine.
- Sulfur plays an important role in protein structure, detoxification reactions, antioxidant defense, and connective tissue formation.
Biochemical Functions of Sulfur
- Constituent of sulfur-containing amino acids (methionine and cysteine).
- Essential for protein synthesis and structure.
- Component of vitamins such as thiamine (Vitamin B₁) and biotin (Vitamin B₇).
- Required for the synthesis of glutathione, an important antioxidant.
- Participates in detoxification reactions in the liver through sulfation.
- Important for the structure of connective tissues, cartilage, skin, hair, and nails.
- Involved in enzyme activity and metabolic reactions.
- Helps maintain normal cellular function and growth.
Dietary Requirement of Sulfur
There is no specific Recommended Dietary Allowance (RDA) for sulfur.
Sulfur requirements are generally met through adequate intake of sulfur-containing amino acids from dietary proteins.
Estimated Requirement
| Nutrient Source | Requirement |
|---|---|
| Methionine + Cysteine | Approximately 13–15 mg/kg body weight/day |
Sources of Sulfur
Sulfur is widely distributed in protein-rich foods.
| Food Source | Sulfur Content |
|---|---|
| Eggs | Rich source |
| Milk and Dairy Products | Rich source |
| Meat and Fish | Rich source |
| Poultry | Rich source |
| Legumes and Pulses | Good source |
| Nuts and Seeds | Good source |
| Garlic and Onion | Rich source |
| Cabbage, Broccoli, Cauliflower | Good source |
| Soy Products | Good source |
Absorption of Sulfur
Sulfur is absorbed primarily in the form of sulfur-containing amino acids.
Mechanism of Absorption
- Methionine and cysteine are absorbed in the small intestine.
- Sulfate ions present in food and water may also be absorbed.
- Absorption occurs mainly in the jejunum and ileum.
Normally, sulfur-containing amino acids are efficiently absorbed from the gastrointestinal tract.
Factors Promoting Sulfur Absorption
| Factor | Mechanism |
|---|---|
| Adequate Protein Intake | Provides sulfur-containing amino acids |
| Healthy Gastrointestinal Function | Ensures efficient absorption |
| Balanced Nutrition | Supports sulfur metabolism |
| Normal Liver Function | Facilitates sulfur utilization |
Factors Inhibiting Sulfur Absorption
| Factor | Mechanism |
|---|---|
| Protein Malnutrition | Decreased sulfur amino acid intake |
| Malabsorption Syndromes | Reduced intestinal absorption |
| Chronic Gastrointestinal Disease | Impaired nutrient uptake |
| Severe Liver Disease | Altered sulfur metabolism |
Sulfur Metabolism
Sulfur metabolism primarily involves:
- Methionine metabolism
- Transsulfuration pathway
- Glutathione synthesis
- Sulfation reactions in the liver
Sulfur is excreted mainly as sulfate in urine.
Disease States Associated with Sulfur Metabolism
1. Sulfur Amino Acid Deficiency
Causes
- Protein-energy malnutrition
- Inadequate dietary protein intake
- Malabsorption disorders
Clinical Features
- Poor growth
- Muscle wasting
- Impaired immunity
- Delayed wound healing
2. Homocystinuria
A genetic disorder of methionine metabolism.
Causes
- Deficiency of cystathionine β-synthase enzyme
Clinical Features
- Developmental delay
- Lens dislocation
- Skeletal abnormalities
- Increased risk of thrombosis
3. Cystinuria
An inherited disorder affecting renal tubular reabsorption of cystine.
Clinical Features
- Recurrent kidney stones
- Hematuria
- Urinary tract obstruction
4. Glutathione Deficiency
Effects
- Increased oxidative stress
- Cellular damage
- Reduced antioxidant protection
| Disorder | Major Defect | Clinical Manifestation |
|---|---|---|
| Sulfur Amino Acid Deficiency | Inadequate intake | Growth retardation, poor immunity |
| Homocystinuria | Methionine metabolism defect | Skeletal and vascular abnormalities |
| Cystinuria | Defective cystine transport | Kidney stone formation |
| Glutathione Deficiency | Reduced antioxidant synthesis | Oxidative stress |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Plasma Homocysteine | Evaluation of homocystinuria |
| Urinary Cystine | Diagnosis of cystinuria |
| Plasma Methionine | Assessment of sulfur amino acid metabolism |
| Glutathione Levels | Evaluation of antioxidant status |
| Liver Function Tests | Assessment of sulfur metabolism |
Microminerals
Iron
Introduction
- Iron is an essential trace element required for oxygen transport, cellular respiration, DNA synthesis, and numerous metabolic processes.
- An adult human body contains approximately 3–5 g of iron, of which about 65–70% is present in hemoglobin, 10% in myoglobin, and the remainder is stored as ferritin and hemosiderin.
- Iron homeostasis is tightly regulated because both iron deficiency and iron overload can lead to significant clinical disorders.
Biochemical Functions of Iron
- Essential component of hemoglobin for oxygen transport.
- Constituent of myoglobin in muscle tissue.
- Participates in electron transport through cytochromes.
- Required for cellular respiration and ATP production.
- Involved in DNA synthesis and cell division.
- Functions as a cofactor for various enzymes.
- Supports immune function and cognitive development.
- Plays a role in detoxification reactions.
Distribution of Iron in the Body
| Site | Percentage |
|---|---|
| Hemoglobin | 65–70% |
| Ferritin and Hemosiderin (Storage Iron) | 20–30% |
| Myoglobin | 3–5% |
| Enzymes and Cytochromes | 1–2% |
| Plasma Transferrin | <1% |
Dietary Requirement of Iron
| Age Group | Requirement (mg/day) |
|---|---|
| Children (1–8 years) | 7–10 |
| Adolescents | 11–15 |
| Adult Men | 8–10 |
| Adult Women | 18 |
| Pregnant Women | 27 |
| Lactating Women | 9–10 |
Sources of Iron
Iron is available in two forms:
Heme Iron
- Derived from animal foods.
- Better absorbed (15–35%).
Non-Heme Iron
- Derived from plant foods.
- Less efficiently absorbed (2–10%).
| Food Source | Type |
|---|---|
| Liver | Heme iron |
| Meat and Poultry | Heme iron |
| Fish | Heme iron |
| Egg Yolk | Heme iron |
| Green Leafy Vegetables | Non-heme iron |
| Legumes and Pulses | Non-heme iron |
| Whole Grains | Non-heme iron |
| Nuts and Seeds | Non-heme iron |
| Jaggery | Non-heme iron |
Absorption of Iron
Iron absorption occurs mainly in the duodenum and upper jejunum.
Mechanism of Absorption
Heme Iron Absorption
- Absorbed intact through heme transporters.
- More efficiently absorbed.
Non-Heme Iron Absorption
- Ferric iron (Fe³⁺) is reduced to ferrous iron (Fe²⁺).
- Ferrous iron is absorbed through DMT1 (Divalent Metal Transporter 1).
Normally, 5–15% of dietary iron is absorbed, depending on body iron stores and dietary factors.
Factors Promoting Iron Absorption
| Factor | Mechanism |
|---|---|
| Vitamin C | Reduces Fe³⁺ to Fe²⁺ |
| Gastric Acid | Maintains iron solubility |
| Heme Iron | Highly bioavailable form |
| Citric Acid | Improves absorption |
| Amino Acids | Enhance iron uptake |
| Iron Deficiency | Increases absorption efficiency |
Factors Inhibiting Iron Absorption
| Factor | Mechanism |
|---|---|
| Phytates (Cereals) | Form insoluble complexes |
| Oxalates | Reduce bioavailability |
| Tannins (Tea, Coffee) | Bind iron |
| Excess Calcium | Interferes with absorption |
| Antacids | Reduce gastric acidity |
| Chronic Intestinal Disease | Impairs absorption |
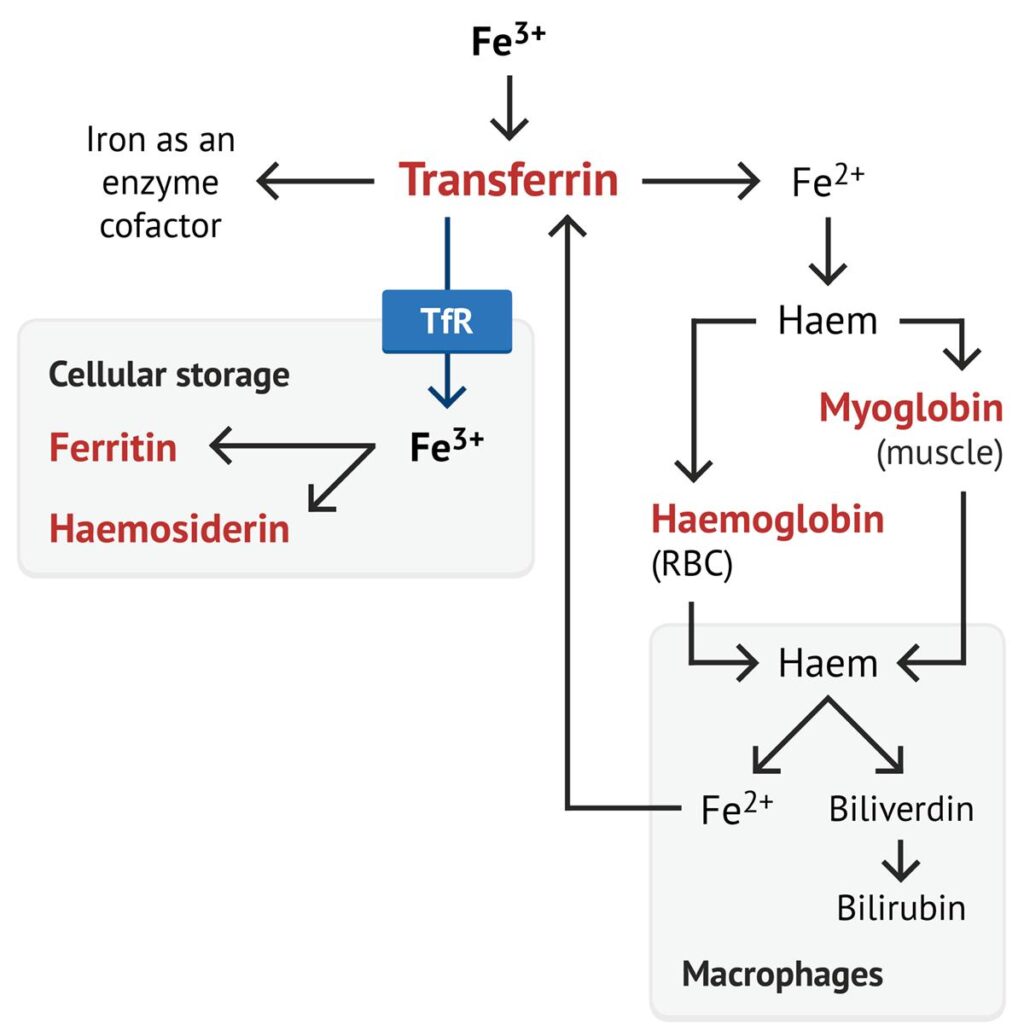
Iron Transport and Storage
Transport
Iron is transported in plasma by transferrin, a glycoprotein synthesized in the liver.
Storage
Iron is stored mainly as:
- Ferritin (soluble storage form)
- Hemosiderin (insoluble storage form)
Storage sites include:
- Liver
- Spleen
- Bone marrow
Regulation of Iron Homeostasis
The key regulator of iron metabolism is hepcidin, a peptide hormone produced by the liver.
Functions of Hepcidin
- Inhibits iron absorption from the intestine.
- Reduces iron release from macrophages.
- Decreases serum iron levels.
Normal Laboratory Values
| Parameter | Reference Range |
|---|---|
| Serum Iron | 60–170 µg/dL |
| Ferritin (Men) | 30–400 ng/mL |
| Ferritin (Women) | 15–150 ng/mL |
| TIBC | 250–450 µg/dL |
| Transferrin Saturation | 20–50% |
Disease States Associated with Iron Metabolism
1. Iron Deficiency Anemia
The most common nutritional deficiency worldwide.
Causes
- Poor dietary intake
- Chronic blood loss
- Malabsorption
- Increased requirements during pregnancy
Clinical Features
- Pallor
- Fatigue
- Weakness
- Shortness of breath
- Koilonychia (spoon-shaped nails)
- Glossitis
2. Iron Overload (Hemochromatosis)
Excessive accumulation of iron in tissues.
Causes
- Hereditary hemochromatosis
- Repeated blood transfusions
Clinical Features
- Liver cirrhosis
- Diabetes mellitus
- Skin pigmentation (“bronze diabetes”)
- Cardiomyopathy
3. Anemia of Chronic Disease
Associated with chronic infections, inflammation, and malignancy.
Mechanism
- Increased hepcidin production
- Reduced iron availability for erythropoiesis
| Disorder | Serum Iron | Ferritin | TIBC |
|---|---|---|---|
| Iron Deficiency Anemia | ↓ | ↓ | ↑ |
| Anemia of Chronic Disease | ↓ | Normal/↑ | ↓ |
| Hemochromatosis | ↑ | ↑ | ↓ |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Hemoglobin | Screening for anemia |
| Serum Iron | Measures circulating iron |
| Ferritin | Best indicator of iron stores |
| TIBC | Measures iron-binding capacity |
| Transferrin Saturation | Assesses iron availability |
| Peripheral Blood Smear | Evaluates RBC morphology |
| Bone Marrow Iron Stain | Gold standard for iron stores |
Copper
Introduction
- Copper is an essential trace element required for numerous biological processes, including iron metabolism, connective tissue formation, antioxidant defense, energy production, and nervous system function.
- An adult human body contains approximately 80–120 mg of copper, with the highest concentrations found in the liver, brain, heart, and kidneys.
- Copper functions primarily as a component of several enzymes and proteins involved in oxidation-reduction reactions.
Biochemical Functions of Copper
- Essential for iron absorption and hemoglobin synthesis.
- Required for the formation of connective tissue, collagen, and elastin.
- Functions as a component of antioxidant enzymes.
- Participates in cellular respiration and energy production.
- Important for normal nervous system function.
- Involved in melanin synthesis and skin pigmentation.
- Supports immune function.
- Plays a role in bone formation and maintenance.
Dietary Requirement of Copper
| Age Group | Requirement (mg/day) |
|---|---|
| Children (1–8 years) | 0.3–0.5 |
| Adolescents | 0.7–0.9 |
| Adult Men | 0.9 |
| Adult Women | 0.9 |
| Pregnant Women | 1.0 |
| Lactating Women | 1.3 |
Sources of Copper
Copper is widely distributed in both plant and animal foods.
| Food Source | Copper Content |
|---|---|
| Liver | Rich source |
| Shellfish | Rich source |
| Nuts and Seeds | Rich source |
| Legumes | Good source |
| Whole Grains | Good source |
| Cocoa and Dark Chocolate | Good source |
| Mushrooms | Moderate source |
| Green Leafy Vegetables | Moderate source |
| Dried Fruits | Moderate source |
Absorption of Copper
Copper is absorbed mainly in the stomach and small intestine, particularly the duodenum.
Mechanism of Absorption
- Dietary copper is released from food in the acidic environment of the stomach.
- Absorbed through intestinal mucosal cells.
- Transported to the liver via the portal circulation.
- Incorporated into ceruloplasmin, the major copper-carrying protein in blood.
Normally, 30–60% of dietary copper is absorbed.
Factors Promoting Copper Absorption
| Factor | Mechanism |
|---|---|
| Adequate Protein Intake | Improves copper utilization |
| Acidic Gastric pH | Enhances copper solubility |
| Normal Intestinal Function | Promotes absorption |
| Balanced Mineral Intake | Supports copper metabolism |
Factors Inhibiting Copper Absorption
| Factor | Mechanism |
|---|---|
| Excess Zinc Intake | Competes with copper absorption |
| High Iron Intake | Reduces copper absorption |
| Antacid Use | Decreases gastric acidity |
| Malabsorption Syndromes | Impairs intestinal uptake |
| Chronic Diarrhea | Increases mineral loss |
Transport and Storage of Copper
Transport
Copper is transported in blood mainly by:
- Ceruloplasmin (90–95%)
- Albumin
- Amino acid complexes
Storage
Copper is stored primarily in:
- Liver
- Brain
- Kidneys
- Heart
Normal Laboratory Values
| Parameter | Reference Range |
|---|---|
| Serum Copper | 70–140 µg/dL |
| Ceruloplasmin | 20–40 mg/dL |
Disease States Associated with Copper Metabolism
1. Copper Deficiency
Causes
- Malnutrition
- Malabsorption syndromes
- Prolonged parenteral nutrition
- Excess zinc supplementation
Clinical Features
- Anemia
- Neutropenia
- Bone abnormalities
- Impaired immunity
- Neurological dysfunction
2. Wilson Disease
An autosomal recessive disorder caused by mutation of the ATP7B gene, resulting in impaired copper excretion.
Features
- Copper accumulation in liver, brain, and cornea.
- Hepatitis and cirrhosis.
- Neurological symptoms.
- Psychiatric disturbances.
- Kayser–Fleischer rings in the cornea.
3. Menkes Disease
A rare X-linked disorder caused by defective copper transport.
Features
- Severe copper deficiency
- Growth retardation
- Neurological deterioration
- Sparse, kinky hair
- Early childhood mortality
| Disorder | Serum Copper | Ceruloplasmin | Major Features |
|---|---|---|---|
| Copper Deficiency | ↓ | ↓ | Anemia, neutropenia |
| Wilson Disease | ↓ | ↓ | Copper accumulation, liver and brain damage |
| Menkes Disease | ↓ | ↓ | Growth failure, neurological defects |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Serum Copper | Evaluates copper status |
| Ceruloplasmin | Major screening test |
| 24-Hour Urinary Copper | Increased in Wilson disease |
| Liver Copper Estimation | Confirms copper overload |
| Genetic Testing | Diagnosis of Wilson and Menkes disease |
Iodine
Introduction
- Iodine is an essential trace element required for the synthesis of thyroid hormones, thyroxine (T₄) and triiodothyronine (T₃).
- These hormones regulate growth, development, metabolism, reproduction, and nervous system function.
- The adult human body contains approximately 15–20 mg of iodine, of which about 70–80% is stored in the thyroid gland.
- Both iodine deficiency and excess can lead to thyroid disorders and significant health problems.
Biochemical Functions of Iodine
- Essential for the synthesis of thyroid hormones (T₃ and T₄).
- Regulates basal metabolic rate (BMR).
- Supports normal growth and development.
- Essential for brain development and cognitive function.
- Regulates protein, carbohydrate, and lipid metabolism.
- Influences body temperature regulation.
- Supports reproductive health and fetal development.
- Maintains normal nervous system function.
Dietary Requirement of Iodine
| Age Group | Requirement (µg/day) |
|---|---|
| Infants (0–12 months) | 110–130 |
| Children (1–8 years) | 90 |
| Children (9–13 years) | 120 |
| Adolescents and Adults | 150 |
| Pregnant Women | 220–250 |
| Lactating Women | 250–290 |
Sources of Iodine
| Food Source | Iodine Content |
|---|---|
| Iodized Salt | Excellent source |
| Marine Fish | Rich source |
| Seaweed | Rich source |
| Shellfish | Rich source |
| Milk and Dairy Products | Good source |
| Eggs | Good source |
| Meat and Poultry | Moderate source |
| Cereals and Grains | Variable source |
Absorption of Iodine
Iodine is absorbed rapidly and almost completely from the gastrointestinal tract.
Mechanism of Absorption
- Dietary iodine is mainly present as iodide (I⁻).
- Absorbed in the stomach and small intestine.
- Transported in blood to the thyroid gland.
- Thyroid follicular cells actively concentrate iodide through the sodium-iodide symporter (NIS).
Normally, more than 90% of dietary iodine is absorbed.
Factors Promoting Iodine Absorption
| Factor | Mechanism |
|---|---|
| Adequate Dietary Intake | Ensures sufficient iodine availability |
| Iodized Salt Consumption | Major source of dietary iodine |
| Healthy Gastrointestinal Function | Promotes efficient absorption |
| Increased Physiological Demand | Enhances iodine utilization |
Factors Inhibiting Iodine Absorption and Utilization
| Factor | Mechanism |
|---|---|
| Iodine Deficient Diet | Reduced intake |
| Goitrogenic Foods* | Interfere with thyroid hormone synthesis |
| Malabsorption Syndromes | Decrease iodine absorption |
| Selenium Deficiency | Impairs thyroid hormone metabolism |
| Excess Nitrates and Thiocyanates | Inhibit iodide uptake by thyroid |
*Goitrogenic foods include cabbage, cauliflower, broccoli, turnip, and millet when consumed in large amounts.
Iodine Metabolism
Steps in Thyroid Hormone Synthesis
- Absorption of iodide from the intestine.
- Active uptake of iodide by thyroid gland.
- Oxidation of iodide to iodine by thyroid peroxidase.
- Iodination of tyrosine residues in thyroglobulin.
- Formation of MIT and DIT.
- Coupling reactions:
- MIT + DIT → T₃
- DIT + DIT → T₄
- Release of T₃ and T₄ into circulation.
Normal Laboratory Values
| Parameter | Reference Range |
|---|---|
| Urinary Iodine | 100–199 µg/L (adequate intake) |
| TSH | 0.4–4.0 mIU/L |
| Free T₄ | 0.8–2.0 ng/dL |
| Free T₃ | 2.3–4.2 pg/mL |
Disease States Associated with Iodine Metabolism
1. Iodine Deficiency Disorders (IDD)
Iodine deficiency is one of the most common micronutrient deficiencies worldwide.
Clinical Manifestations
- Goiter
- Hypothyroidism
- Growth retardation
- Impaired mental development
- Reduced work capacity
2. Endemic Goiter
Enlargement of the thyroid gland caused by inadequate iodine intake.
Features
- Visible neck swelling
- Increased TSH secretion
- Compensatory thyroid enlargement
3. Cretinism
Severe iodine deficiency during fetal life and early childhood.
Clinical Features
- Severe mental retardation
- Deaf-mutism
- Stunted growth
- Delayed sexual development
4. Hypothyroidism
Causes
- Iodine deficiency
- Autoimmune thyroid disease
- Thyroid surgery
Clinical Features
- Fatigue
- Weight gain
- Cold intolerance
- Dry skin
- Constipation
5. Hyperthyroidism (Iodine Excess)
Excess iodine intake may occasionally trigger hyperthyroidism in susceptible individuals.
Clinical Features
- Weight loss
- Heat intolerance
- Palpitations
- Nervousness
- Increased appetite
| Disorder | Iodine Status | Major Features |
|---|---|---|
| Iodine Deficiency | ↓ | Goiter, hypothyroidism |
| Endemic Goiter | ↓ | Thyroid enlargement |
| Cretinism | Severe ↓ | Mental and physical retardation |
| Hypothyroidism | ↓ | Reduced metabolic activity |
| Iodine-Induced Hyperthyroidism | ↑ | Excess thyroid hormone production |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Urinary Iodine Estimation | Best indicator of iodine intake |
| Serum TSH | Screening test for thyroid function |
| Free T₃ and Free T₄ | Assessment of thyroid hormone status |
| Thyroid Ultrasound | Evaluation of goiter |
| Thyroid Antibody Tests | Assessment of autoimmune thyroid disease |
Manganese
Introduction
- Manganese is an essential trace element required for normal growth, bone formation, reproduction, and metabolism.
- It acts as a cofactor for several enzymes involved in carbohydrate, lipid, protein, and antioxidant metabolism.
- The adult human body contains approximately 10–20 mg of manganese, with the highest concentrations found in the liver, pancreas, kidneys, and bones.
- Although required only in small amounts, manganese is vital for maintaining normal physiological functions.
Biochemical Functions of Manganese
- Acts as a cofactor for numerous enzymes.
- Essential for carbohydrate, protein, and lipid metabolism.
- Required for bone formation and skeletal development.
- Participates in collagen synthesis and wound healing.
- Supports normal reproductive function.
- Important for nervous system function.
- Component of manganese superoxide dismutase (Mn-SOD), an important antioxidant enzyme.
- Involved in the synthesis of mucopolysaccharides and connective tissue.
Dietary Requirement of Manganese
| Age Group | Requirement (mg/day) |
|---|---|
| Children (1–8 years) | 1.2–1.5 |
| Adolescents | 1.6–2.2 |
| Adult Men | 2.3 |
| Adult Women | 1.8 |
| Pregnant Women | 2.0 |
| Lactating Women | 2.6 |
Sources of Manganese
Manganese is widely distributed in plant-based foods.
| Food Source | Manganese Content |
|---|---|
| Whole Grains | Rich source |
| Nuts (Almonds, Walnuts) | Rich source |
| Legumes and Pulses | Rich source |
| Tea | Rich source |
| Green Leafy Vegetables | Good source |
| Brown Rice | Good source |
| Pineapple | Moderate source |
| Soy Products | Good source |
| Spices | Rich source |
Absorption of Manganese
Manganese is absorbed mainly in the small intestine, particularly the duodenum and jejunum.
Mechanism of Absorption
- Absorbed through active and passive transport mechanisms.
- Transported in blood bound to transferrin, albumin, and other plasma proteins.
- Excess manganese is excreted mainly through bile.
Normally, only 3–5% of dietary manganese is absorbed.
Factors Promoting Manganese Absorption
| Factor | Mechanism |
|---|---|
| Adequate Dietary Intake | Maintains manganese stores |
| Iron Deficiency | Increases manganese absorption |
| Healthy Intestinal Function | Promotes efficient uptake |
| Balanced Nutrition | Supports mineral metabolism |
Factors Inhibiting Manganese Absorption
| Factor | Mechanism |
|---|---|
| Excess Iron Intake | Competes for absorption |
| Excess Calcium Intake | Reduces manganese uptake |
| High Phosphate Intake | Decreases absorption |
| Malabsorption Syndromes | Impairs intestinal uptake |
| Chronic Gastrointestinal Disorders | Reduce absorption efficiency |
Manganese Homeostasis
Manganese balance is regulated mainly by:
- Intestinal absorption
- Hepatic storage
- Biliary excretion
The liver plays a central role in maintaining manganese homeostasis.
Normal Laboratory Values
| Parameter | Reference Range |
|---|---|
| Serum Manganese | 4–15 µg/L |
Disease States Associated with Manganese Metabolism
1. Manganese Deficiency
Manganese deficiency is uncommon but may occur in severe malnutrition or prolonged parenteral nutrition.
Clinical Features
- Impaired growth
- Skeletal abnormalities
- Reduced fertility
- Poor wound healing
- Altered carbohydrate metabolism
2. Manganese Toxicity (Manganism)
Excess manganese accumulation can occur due to occupational exposure, liver disease, or excessive supplementation.
Causes
- Mining and welding industries
- Environmental exposure
- Chronic liver disease
Clinical Features
- Tremors
- Muscle rigidity
- Difficulty walking
- Parkinson-like symptoms
- Behavioral changes
| Disorder | Manganese Status | Major Features |
|---|---|---|
| Manganese Deficiency | ↓ | Growth retardation, skeletal defects |
| Manganese Toxicity (Manganism) | ↑ | Neurological and Parkinson-like symptoms |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Serum Manganese | Assessment of manganese status |
| Whole Blood Manganese | Evaluation of chronic exposure |
| Liver Function Tests | Assessment of manganese excretion |
| MRI Brain | Detection of manganese accumulation in toxicity |
Zinc
Introduction
- Zinc is an essential trace element that plays a crucial role in growth, development, immune function, wound healing, and cellular metabolism.
- It is the second most abundant trace element in the body after iron.
- An adult human body contains approximately 2–3 g of zinc, with the highest concentrations found in skeletal muscle, bones, skin, liver, and prostate gland.
- Zinc acts as a structural, catalytic, and regulatory component of more than 300 enzymes and numerous transcription factors.
Biochemical Functions of Zinc
- Acts as a cofactor for more than 300 enzymes.
- Essential for DNA and RNA synthesis.
- Required for protein synthesis and cell division.
- Supports normal growth and development.
- Maintains immune function.
- Promotes wound healing.
- Important for taste and smell perception.
- Involved in reproductive function and fertility.
- Functions as an antioxidant by stabilizing cell membranes.
- Regulates gene expression through zinc-finger proteins.
Dietary Requirement of Zinc
| Age Group | Requirement (mg/day) |
|---|---|
| Children (1–8 years) | 3–5 |
| Adolescents | 8–11 |
| Adult Men | 11 |
| Adult Women | 8 |
| Pregnant Women | 11–12 |
| Lactating Women | 12–13 |
Sources of Zinc
Zinc is widely distributed in both animal and plant foods.
| Food Source | Zinc Content |
|---|---|
| Oysters and Shellfish | Excellent source |
| Meat and Poultry | Rich source |
| Fish | Good source |
| Eggs | Good source |
| Milk and Dairy Products | Moderate source |
| Legumes and Pulses | Good source |
| Nuts and Seeds | Good source |
| Whole Grains | Moderate source |
| Soy Products | Good source |
Absorption of Zinc
Zinc is absorbed mainly in the duodenum and jejunum.
Mechanism of Absorption
- Absorbed through specialized zinc transport proteins.
- Transported in plasma mainly bound to albumin.
- Excess zinc is excreted primarily through feces.
Normally, 20–40% of dietary zinc is absorbed.
Factors Promoting Zinc Absorption
| Factor | Mechanism |
|---|---|
| Animal Protein | Improves zinc bioavailability |
| Organic Acids | Increase zinc solubility |
| Adequate Dietary Intake | Maintains zinc stores |
| Healthy Intestinal Function | Promotes efficient absorption |
Factors Inhibiting Zinc Absorption
| Factor | Mechanism |
|---|---|
| Phytates (Whole Grains, Cereals) | Bind zinc and reduce absorption |
| Excess Calcium | May interfere with absorption |
| Excess Iron Supplementation | Competes for absorption |
| High Dietary Fiber | Decreases bioavailability |
| Malabsorption Syndromes | Reduce intestinal uptake |
Zinc Homeostasis
Zinc balance is maintained through:
- Intestinal absorption
- Tissue storage
- Fecal excretion
Unlike iron, the body has limited zinc storage capacity, making regular dietary intake essential.
Normal Laboratory Values
| Parameter | Reference Range |
|---|---|
| Serum Zinc | 70–120 µg/dL |
Disease States Associated with Zinc Metabolism
1. Zinc Deficiency
Zinc deficiency is one of the most common micronutrient deficiencies worldwide.
Causes
- Poor dietary intake
- Malnutrition
- Malabsorption syndromes
- Chronic diarrhea
- Increased physiological requirements
Clinical Features
- Growth retardation
- Delayed sexual maturation
- Impaired immunity
- Delayed wound healing
- Hair loss (alopecia)
- Loss of taste (hypogeusia)
- Skin lesions and dermatitis
2. Acrodermatitis Enteropathica
A rare inherited disorder caused by defective intestinal zinc absorption.
Clinical Features
- Severe zinc deficiency
- Periorificial dermatitis
- Diarrhea
- Alopecia
- Growth retardation
3. Zinc Toxicity
Usually occurs due to excessive supplementation.
Clinical Features
- Nausea and vomiting
- Abdominal pain
- Diarrhea
- Copper deficiency
- Impaired immune function
| Disorder | Zinc Status | Major Features |
|---|---|---|
| Zinc Deficiency | ↓ | Growth retardation, impaired immunity |
| Acrodermatitis Enteropathica | ↓ | Dermatitis, diarrhea, alopecia |
| Zinc Toxicity | ↑ | Gastrointestinal symptoms, copper deficiency |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Serum Zinc | Primary assessment of zinc status |
| Plasma Zinc | Evaluation of deficiency |
| Alkaline Phosphatase Activity | May decrease in zinc deficiency |
| Hair Zinc Analysis | Assessment of long-term status |
| Dietary Assessment | Evaluation of zinc intake |
Molybdenum
Introduction
- Molybdenum is an essential trace element required in very small amounts for normal human health.
- It functions primarily as a cofactor for several enzymes involved in the metabolism of sulfur-containing amino acids, purines, pyrimidines, and various toxic compounds.
- The total body content of molybdenum is approximately 5–10 mg, with the highest concentrations found in the liver, kidneys, and bones.
- Although molybdenum deficiency is rare, it is essential for several critical biochemical reactions.
Biochemical Functions of Molybdenum
- Acts as a cofactor for important enzymes.
- Essential for sulfur amino acid metabolism.
- Involved in purine degradation and uric acid formation.
- Participates in detoxification of sulfites.
- Supports metabolism of drugs and toxins.
- Plays a role in cellular oxidation-reduction reactions.
Important Molybdenum-Dependent Enzymes
| Enzyme | Function |
|---|---|
| Xanthine Oxidase | Converts hypoxanthine → xanthine → uric acid |
| Sulfite Oxidase | Converts sulfite to sulfate |
| Aldehyde Oxidase | Metabolism of aldehydes and drugs |
| Mitochondrial Amidoxime Reducing Component (mARC) | Detoxification reactions |
Dietary Requirement of Molybdenum
| Age Group | Requirement (µg/day) |
|---|---|
| Children (1–8 years) | 17–22 |
| Adolescents | 34–43 |
| Adult Men | 45 |
| Adult Women | 45 |
| Pregnant Women | 50 |
| Lactating Women | 50 |
Sources of Molybdenum
Molybdenum is widely distributed in foods, especially legumes and cereals.
| Food Source | Molybdenum Content |
|---|---|
| Legumes (Beans, Lentils, Peas) | Rich source |
| Whole Grains | Rich source |
| Nuts | Good source |
| Green Leafy Vegetables | Moderate source |
| Milk and Dairy Products | Moderate source |
| Liver and Kidney | Good source |
| Eggs | Moderate source |
Absorption of Molybdenum
Molybdenum is absorbed efficiently from the gastrointestinal tract, mainly as molybdate ions (MoO₄²⁻).
Mechanism of Absorption
- Absorbed in the stomach and small intestine.
- Transported in blood as molybdate.
- Stored mainly in the liver and kidneys.
- Excess molybdenum is excreted through urine.
Normally, 50–90% of dietary molybdenum is absorbed.
Factors Promoting Molybdenum Absorption
| Factor | Mechanism |
|---|---|
| Adequate Dietary Intake | Maintains body stores |
| Healthy Intestinal Function | Promotes efficient absorption |
| Balanced Nutrition | Supports trace element metabolism |
Factors Inhibiting Molybdenum Absorption
| Factor | Mechanism |
|---|---|
| Malabsorption Syndromes | Impaired intestinal uptake |
| Chronic Gastrointestinal Disorders | Reduced absorption |
| Excess Copper Intake | May interfere with molybdenum utilization |
Normal Laboratory Values
Routine assessment of molybdenum status is rarely performed.
| Parameter | Reference Range |
|---|---|
| Plasma Molybdenum | 0.3–1.5 µg/L |
Disease States Associated with Molybdenum Metabolism
1. Molybdenum Deficiency
Molybdenum deficiency is extremely rare and is usually seen in individuals receiving long-term parenteral nutrition without adequate supplementation.
Clinical Features
- Neurological abnormalities
- Headache
- Tachycardia
- Mental confusion
- Sulfite toxicity
2. Molybdenum Cofactor Deficiency
A rare inherited metabolic disorder characterized by deficiency of all molybdenum-dependent enzymes.
Clinical Features
- Severe neurological impairment
- Developmental delay
- Seizures
- Feeding difficulties
- Early childhood mortality
3. Molybdenum Toxicity
Usually uncommon but may occur due to excessive environmental or occupational exposure.
Clinical Features
- Increased uric acid levels
- Joint pain resembling gout
- Gastrointestinal disturbances
| Disorder | Molybdenum Status | Major Features |
|---|---|---|
| Molybdenum Deficiency | ↓ | Neurological abnormalities |
| Molybdenum Cofactor Deficiency | Functional deficiency | Seizures, developmental delay |
| Molybdenum Toxicity | ↑ | Hyperuricemia, gout-like symptoms |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Plasma Molybdenum | Assessment of molybdenum levels |
| Urinary Sulfite | Elevated in sulfite oxidase deficiency |
| Serum Uric Acid | May increase in toxicity |
| Genetic Testing | Diagnosis of molybdenum cofactor deficiency |
Cobalt
Introduction
- Cobalt is an essential trace element that is primarily important as a constituent of Vitamin B₁₂ (Cobalamin).
- Unlike many other trace elements, cobalt does not have a significant independent metabolic role in humans apart from its incorporation into Vitamin B₁₂.
- It is required for normal red blood cell formation, DNA synthesis, neurological function, and cellular metabolism.
- The total body content of cobalt is very small, approximately 1–2 mg, most of which is present as part of Vitamin B₁₂ stored in the liver.
Biochemical Functions of Cobalt
- Essential component of Vitamin B₁₂ (Cobalamin).
- Required for red blood cell formation.
- Necessary for DNA synthesis and cell division.
- Supports normal nervous system function.
- Participates in amino acid metabolism.
- Involved in fatty acid metabolism.
- Helps maintain normal growth and development.
Dietary Requirement of Cobalt
There is no separate Recommended Dietary Allowance (RDA) for cobalt because its requirement is met through Vitamin B₁₂ intake.
| Age Group | Vitamin B₁₂ Requirement (µg/day) |
|---|---|
| Children (1–8 years) | 0.9–1.2 |
| Adolescents | 1.8–2.4 |
| Adult Men | 2.4 |
| Adult Women | 2.4 |
| Pregnant Women | 2.6 |
| Lactating Women | 2.8 |
Sources of Cobalt
Since cobalt is present mainly as part of Vitamin B₁₂, its sources are primarily animal foods.
| Food Source | Cobalt Source |
|---|---|
| Liver | Rich source |
| Meat and Poultry | Rich source |
| Fish and Seafood | Rich source |
| Eggs | Good source |
| Milk and Dairy Products | Good source |
| Fortified Cereals | Source of Vitamin B₁₂ |
| Nutritional Supplements | Variable source |
Note: Strict vegetarians and vegans may be at risk of Vitamin B₁₂ deficiency unless they consume fortified foods or supplements.
Absorption of Cobalt
Cobalt is absorbed indirectly as part of Vitamin B₁₂.
Mechanism of Absorption
- Vitamin B₁₂ is released from food in the stomach.
- It binds to intrinsic factor secreted by gastric parietal cells.
- The Vitamin B₁₂–intrinsic factor complex is absorbed in the terminal ileum.
- Vitamin B₁₂ is transported in blood by transcobalamin proteins.
- Excess cobalt is excreted mainly through urine.
Factors Promoting Cobalt Absorption
| Factor | Mechanism |
|---|---|
| Adequate Intrinsic Factor | Essential for Vitamin B₁₂ absorption |
| Healthy Ileum | Site of Vitamin B₁₂ uptake |
| Adequate Dietary Vitamin B₁₂ | Maintains body stores |
| Normal Gastric Function | Facilitates Vitamin B₁₂ release from food |
Factors Inhibiting Cobalt Absorption
| Factor | Mechanism |
|---|---|
| Pernicious Anemia | Lack of intrinsic factor |
| Ileal Disease or Resection | Impaired absorption |
| Chronic Gastritis | Reduced Vitamin B₁₂ release |
| Strict Vegan Diet | Low Vitamin B₁₂ intake |
| Malabsorption Syndromes | Reduced intestinal uptake |
Normal Laboratory Values
Routine cobalt estimation is rarely performed.
| Parameter | Reference Range |
|---|---|
| Serum Vitamin B₁₂ | 200–900 pg/mL |
Disease States Associated with Cobalt Metabolism
1. Vitamin B₁₂ Deficiency
Since cobalt functions mainly through Vitamin B₁₂, deficiency manifestations are essentially those of cobalamin deficiency.
Causes
- Pernicious anemia
- Malabsorption syndromes
- Strict vegetarian or vegan diet
- Gastric surgery
- Ileal disease
Clinical Features
- Megaloblastic anemia
- Fatigue and weakness
- Glossitis
- Peripheral neuropathy
- Memory impairment
- Subacute combined degeneration of the spinal cord
2. Pernicious Anemia
An autoimmune disorder characterized by intrinsic factor deficiency.
Features
- Vitamin B₁₂ malabsorption
- Megaloblastic anemia
- Neurological manifestations
3. Cobalt Toxicity
Rare and usually associated with occupational exposure or excessive supplementation.
Clinical Features
- Cardiomyopathy
- Polycythemia
- Thyroid dysfunction
- Neurological symptoms
| Disorder | Major Defect | Clinical Features |
|---|---|---|
| Vitamin B₁₂ Deficiency | Inadequate cobalamin | Megaloblastic anemia, neuropathy |
| Pernicious Anemia | Intrinsic factor deficiency | Vitamin B₁₂ malabsorption |
| Cobalt Toxicity | Excess exposure | Cardiomyopathy, polycythemia |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Serum Vitamin B₁₂ | Primary assessment |
| Complete Blood Count (CBC) | Detects megaloblastic anemia |
| Peripheral Blood Smear | Macrocytic RBCs |
| Serum Homocysteine | Elevated in deficiency |
| Serum Methylmalonic Acid | Increased in Vitamin B₁₂ deficiency |
| Intrinsic Factor Antibody Test | Diagnosis of pernicious anemia |
Fluoride
Introduction
- Fluoride is an essential trace element that plays a vital role in the development and maintenance of bones and teeth.
- It is the ionic form of fluorine and is naturally present in water, soil, and various foods.
- Approximately 95–99% of body fluoride is found in bones and teeth, where it helps strengthen the mineral matrix and increases resistance to dental caries.
- Although fluoride is beneficial in small amounts, both deficiency and excess intake can lead to health problems.
Biochemical Functions of Fluoride
- Strengthens tooth enamel by forming fluorapatite.
- Increases resistance of teeth to dental caries.
- Promotes remineralization of tooth enamel.
- Contributes to normal bone mineralization.
- Enhances bone density and skeletal strength.
- Reduces acid dissolution of enamel.
- May inhibit bacterial metabolism in dental plaque.
Dietary Requirement of Fluoride
| Age Group | Requirement (mg/day) |
|---|---|
| Children (1–8 years) | 0.7–1.0 |
| Adolescents | 2–3 |
| Adult Men | 4.0 |
| Adult Women | 3.0 |
| Pregnant Women | 3.0 |
| Lactating Women | 3.0 |
Sources of Fluoride
| Food Source | Fluoride Content |
|---|---|
| Fluoridated Drinking Water | Major source |
| Tea | Rich source |
| Marine Fish | Good source |
| Seafood | Good source |
| Fluoridated Salt | Good source |
| Toothpaste (topical source) | Prevents dental caries |
| Some Vegetables and Fruits | Variable amounts |
Absorption of Fluoride
Fluoride is absorbed rapidly from the gastrointestinal tract.
Mechanism of Absorption
- Absorbed mainly in the stomach and small intestine.
- Transported through blood to bones and teeth.
- Incorporated into hydroxyapatite crystals to form fluorapatite.
- Excess fluoride is excreted primarily through the kidneys.
Normally, 75–90% of ingested fluoride is absorbed.
Factors Promoting Fluoride Absorption
| Factor | Mechanism |
|---|---|
| Acidic Gastric pH | Increases fluoride solubility |
| Fluoridated Water | Provides readily absorbable fluoride |
| Adequate Dietary Intake | Maintains fluoride stores |
| Healthy Gastrointestinal Function | Supports absorption |
Factors Inhibiting Fluoride Absorption
| Factor | Mechanism |
|---|---|
| Calcium-rich Foods | Form insoluble calcium fluoride |
| Magnesium and Aluminum Salts | Reduce fluoride absorption |
| Antacids | Interfere with absorption |
| Malabsorption Syndromes | Decrease intestinal uptake |
Fluoride Metabolism
- Absorbed from the gastrointestinal tract.
- Distributed mainly to bones and teeth.
- Stored as fluorapatite in mineralized tissues.
- Excreted primarily by the kidneys.
- Small amounts are lost through sweat and feces.
Normal Fluoride Levels
| Parameter | Reference Range |
|---|---|
| Serum Fluoride | 0.01–0.05 mg/L |
| Drinking Water Fluoride (Optimal) | 0.7–1.2 mg/L |
Disease States Associated with Fluoride Metabolism
1. Fluoride Deficiency
Causes
- Low fluoride content in drinking water
- Inadequate fluoride intake
Clinical Features
- Increased dental caries
- Weak tooth enamel
- Increased susceptibility to tooth decay
2. Dental Fluorosis
Results from excessive fluoride intake during tooth development.
Clinical Features
- White opaque patches on teeth
- Brown discoloration
- Mottling of enamel
- Enamel pitting in severe cases
3. Skeletal Fluorosis
A chronic condition caused by prolonged excessive fluoride intake.
Causes
- High fluoride concentration in drinking water
- Industrial exposure
Clinical Features
- Joint pain and stiffness
- Osteosclerosis
- Calcification of ligaments
- Restricted joint movement
- Skeletal deformities
| Disorder | Fluoride Status | Major Features |
|---|---|---|
| Fluoride Deficiency | ↓ | Dental caries |
| Dental Fluorosis | ↑ | Mottled and discolored teeth |
| Skeletal Fluorosis | ↑↑ | Bone and joint abnormalities |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Water Fluoride Analysis | Assesses environmental exposure |
| Urinary Fluoride | Best indicator of fluoride intake |
| Serum Fluoride | Evaluation of fluoride status |
| Dental Examination | Detects fluorosis |
| Skeletal X-ray | Diagnosis of skeletal fluorosis |
Selenium
Introduction
- Selenium is an essential trace element required for normal growth, reproduction, thyroid hormone metabolism, and antioxidant defense.
- It is incorporated into a group of proteins known as selenoproteins, which play important roles in protecting cells from oxidative damage.
- The adult human body contains approximately 13–20 mg of selenium, with the highest concentrations found in the liver, kidneys, thyroid gland, and muscles.
- Selenium works synergistically with Vitamin E to maintain cellular integrity and immune function.
Biochemical Functions of Selenium
- Component of antioxidant enzymes such as glutathione peroxidase.
- Protects cells against oxidative stress and free radical damage.
- Essential for thyroid hormone metabolism.
- Supports immune system function.
- Plays a role in reproduction and fertility.
- Helps maintain cardiovascular health.
- Participates in DNA synthesis and cellular growth.
- Supports normal muscle function.
Dietary Requirement of Selenium
| Age Group | Requirement (µg/day) |
|---|---|
| Children (1–8 years) | 20–30 |
| Adolescents | 40–55 |
| Adult Men | 55 |
| Adult Women | 55 |
| Pregnant Women | 60 |
| Lactating Women | 70 |
Sources of Selenium
Selenium content of foods depends largely on the selenium content of soil.
| Food Source | Selenium Content |
|---|---|
| Brazil Nuts | Excellent source |
| Fish and Seafood | Rich source |
| Meat and Poultry | Rich source |
| Eggs | Good source |
| Milk and Dairy Products | Good source |
| Whole Grains | Moderate source |
| Legumes | Moderate source |
| Mushrooms | Moderate source |
Absorption of Selenium
Selenium is absorbed mainly in the small intestine.
Mechanism of Absorption
- Organic forms (selenomethionine and selenocysteine) are absorbed efficiently.
- Inorganic forms (selenite and selenate) are also absorbed readily.
- Transported in plasma bound to proteins.
- Stored mainly in the liver, kidneys, muscles, and thyroid gland.
Normally, 70–90% of dietary selenium is absorbed.
Factors Promoting Selenium Absorption
| Factor | Mechanism |
|---|---|
| Adequate Dietary Protein | Improves selenium utilization |
| Organic Selenium Sources | Better bioavailability |
| Healthy Intestinal Function | Promotes absorption |
| Balanced Nutrition | Supports selenium metabolism |
Factors Inhibiting Selenium Absorption
| Factor | Mechanism |
|---|---|
| Malabsorption Syndromes | Reduced intestinal uptake |
| Chronic Gastrointestinal Disease | Decreased absorption |
| Severe Protein Deficiency | Impaired selenium utilization |
| Heavy Metal Exposure | May interfere with selenium metabolism |
Selenium-Dependent Enzymes
| Enzyme/Protein | Function |
|---|---|
| Glutathione Peroxidase | Antioxidant protection |
| Thioredoxin Reductase | Cellular redox regulation |
| Iodothyronine Deiodinase | Conversion of T₄ to T₃ |
| Selenoprotein P | Selenium transport and antioxidant activity |
Normal Laboratory Values
| Parameter | Reference Range |
|---|---|
| Serum Selenium | 70–150 µg/L |
Disease States Associated with Selenium Metabolism
1. Selenium Deficiency
Causes
- Poor dietary intake
- Malnutrition
- Long-term parenteral nutrition without supplementation
- Malabsorption syndromes
Clinical Features
- Muscle weakness
- Fatigue
- Impaired immunity
- Thyroid dysfunction
- Cardiomyopathy
2. Keshan Disease
An endemic cardiomyopathy associated with severe selenium deficiency.
Clinical Features
- Cardiac enlargement
- Heart failure
- Arrhythmias
- Increased mortality
3. Kashin-Beck Disease
A chronic osteoarthropathy associated with selenium deficiency.
Clinical Features
- Joint deformities
- Growth retardation
- Skeletal abnormalities
4. Selenium Toxicity (Selenosis)
Occurs due to excessive selenium intake.
Clinical Features
- Hair loss
- Brittle nails
- Garlic-like breath odor
- Gastrointestinal disturbances
- Neurological abnormalities
| Disorder | Selenium Status | Major Features |
|---|---|---|
| Selenium Deficiency | ↓ | Weakness, impaired immunity |
| Keshan Disease | Severe ↓ | Cardiomyopathy |
| Kashin-Beck Disease | ↓ | Osteoarthropathy |
| Selenosis | ↑ | Hair loss, nail changes |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Serum Selenium | Assessment of selenium status |
| Plasma Glutathione Peroxidase Activity | Functional indicator |
| Thyroid Function Tests | Evaluation of thyroid effects |
| Hair and Nail Selenium Analysis | Long-term selenium exposure |
Chromium
Introduction
- Chromium is an essential trace element that plays an important role in carbohydrate, lipid, and protein metabolism.
- It enhances the action of insulin and is therefore involved in maintaining normal glucose homeostasis.
- The total body content of chromium is approximately 4–6 mg, with small amounts distributed in the liver, kidneys, spleen, bones, and soft tissues.
- Chromium exists primarily in the trivalent form (Cr³⁺), which is the biologically active and nutritionally important form.
Biochemical Functions of Chromium
- Enhances the action of insulin.
- Helps regulate blood glucose levels.
- Participates in carbohydrate metabolism.
- Involved in lipid metabolism.
- Supports protein metabolism.
- Facilitates cellular uptake of glucose.
- Contributes to energy production.
- May help maintain normal cholesterol levels.
Dietary Requirement of Chromium
| Age Group | Requirement (µg/day) |
|---|---|
| Children (1–8 years) | 11–15 |
| Adolescents | 21–35 |
| Adult Men | 35 |
| Adult Women | 25 |
| Pregnant Women | 30 |
| Lactating Women | 45 |
Sources of Chromium
Chromium is widely distributed in foods, although the concentration varies depending on soil content and food processing.
| Food Source | Chromium Content |
|---|---|
| Whole Grains | Good source |
| Broccoli | Rich source |
| Nuts | Good source |
| Legumes | Good source |
| Meat and Poultry | Moderate source |
| Eggs | Moderate source |
| Brewer’s Yeast | Rich source |
| Mushrooms | Good source |
| Potatoes | Moderate source |
Absorption of Chromium
Chromium is absorbed mainly in the small intestine.
Mechanism of Absorption
- Absorbed in the trivalent form (Cr³⁺).
- Transported in blood bound mainly to transferrin and albumin.
- Stored in small amounts in tissues.
- Excess chromium is excreted through urine.
Normally, only 0.5–2% of dietary chromium is absorbed.
Factors Promoting Chromium Absorption
| Factor | Mechanism |
|---|---|
| Vitamin C | Improves chromium absorption |
| Niacin (Vitamin B₃) | Enhances chromium utilization |
| Adequate Dietary Intake | Maintains body stores |
| Healthy Intestinal Function | Supports absorption |
Factors Inhibiting Chromium Absorption
| Factor | Mechanism |
|---|---|
| High Intake of Simple Sugars | Increases chromium loss |
| Excess Zinc or Iron | May interfere with absorption |
| Antacid Use | May reduce absorption |
| Malabsorption Syndromes | Impaired intestinal uptake |
| Aging | Reduced chromium absorption |
Chromium Homeostasis
Chromium balance is maintained through:
- Intestinal absorption
- Tissue storage
- Renal excretion
The kidneys are the primary route of chromium elimination.
Normal Laboratory Values
Table 6. Normal Chromium Levels
| Parameter | Reference Range |
|---|---|
| Serum Chromium | 0.1–0.5 µg/L |
Disease States Associated with Chromium Metabolism
1. Chromium Deficiency
Chromium deficiency is uncommon but may occur in malnutrition or prolonged total parenteral nutrition.
Causes
- Inadequate dietary intake
- Long-term parenteral nutrition
- Malabsorption disorders
- Increased urinary losses
Clinical Features
- Impaired glucose tolerance
- Insulin resistance
- Hyperglycemia
- Peripheral neuropathy
- Weight loss
2. Chromium Toxicity
Toxicity from dietary chromium is rare.
Causes
- Excessive supplementation
- Occupational exposure to chromium compounds
Clinical Features
- Gastrointestinal irritation
- Liver dysfunction
- Kidney damage
- Skin reactions
| Disorder | Chromium Status | Major Features |
|---|---|---|
| Chromium Deficiency | ↓ | Impaired glucose tolerance, insulin resistance |
| Chromium Toxicity | ↑ | Renal and hepatic damage |
Laboratory Investigations
| Test | Clinical Significance |
|---|---|
| Serum Chromium | Assessment of chromium status |
| Urinary Chromium | Evaluation of chromium exposure |
| Blood Glucose | Assessment of metabolic effects |
| HbA1c | Long-term glucose control |
| Renal Function Tests | Evaluation of toxicity |

