Introduction
- Branched-Chain Amino Acid Metabolism consist of three essential amino acids: Leucine, Isoleucine, and Valine.
- They cannot be synthesized by the body and must be obtained from the diet.
- They possess branched aliphatic side chains, which give them their name.
- BCAAs account for about 35–40% of essential amino acids in body proteins.
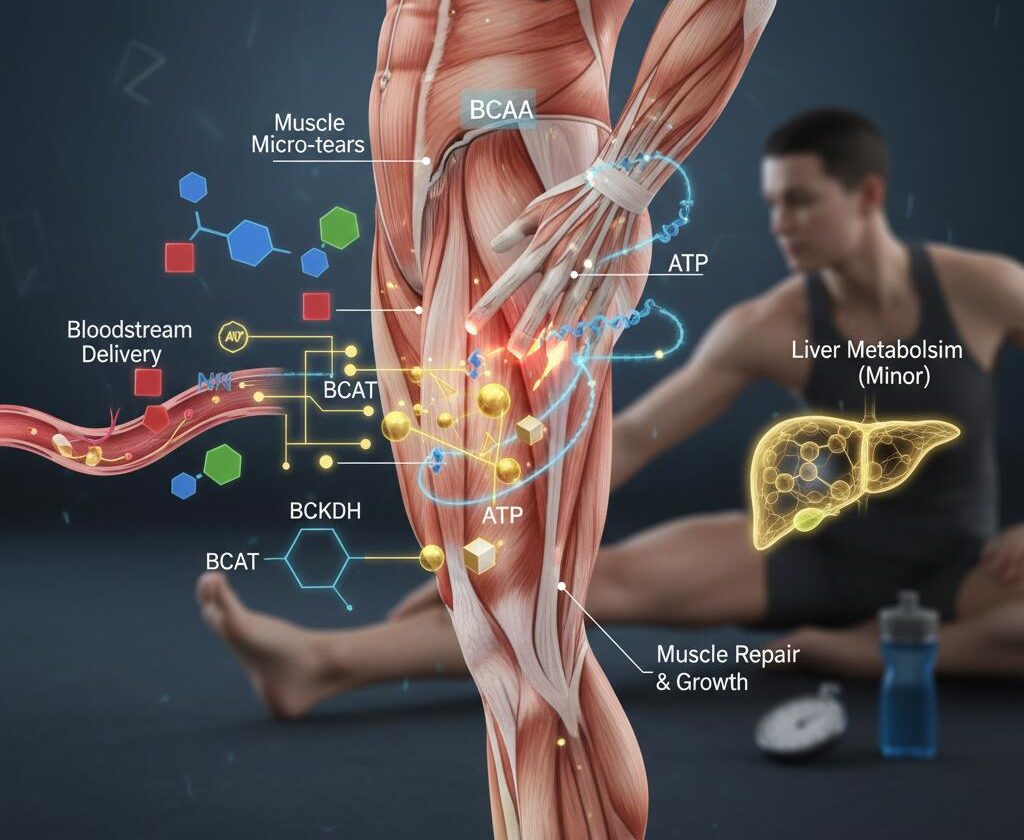
- Unlike most amino acids, BCAAs are primarily metabolized in skeletal muscle, not the liver.
- Leucine stimulates muscle protein synthesis through activation of the mTOR pathway.
- BCAAs serve as an important energy source during prolonged exercise and fasting.
- They help maintain nitrogen balance and support immune function.
- Abnormal BCAA metabolism is associated with obesity, insulin resistance, and type 2 diabetes mellitus.
- Deficiency of BCAA-metabolizing enzymes causes Maple Syrup Urine Disease (MSUD), a serious inherited metabolic disorder.
What Are Branched-Chain Amino Acids?
Branched-chain amino acids are essential amino acids that cannot be synthesized by the human body and must therefore be obtained through dietary sources.
The three BCAAs include:
Leucine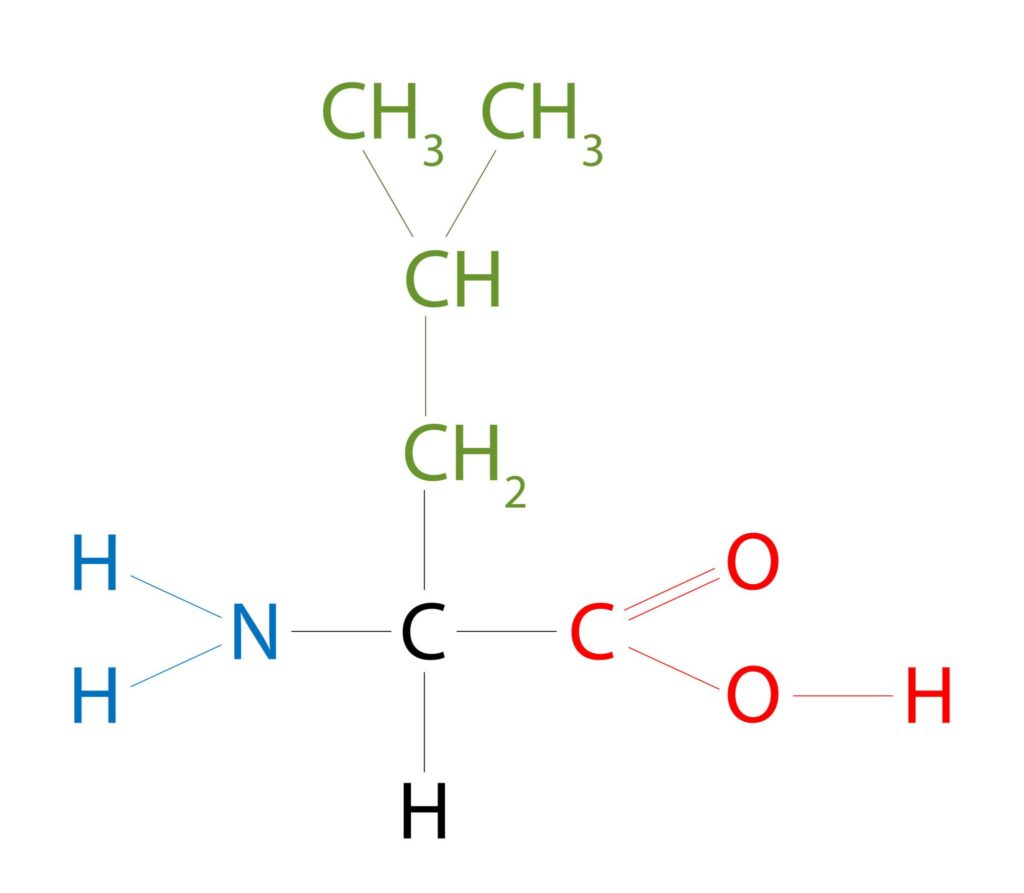
Leucine is the most metabolically active BCAA and serves as a potent stimulator of protein synthesis through activation of the mTOR signaling pathway.
Isoleucine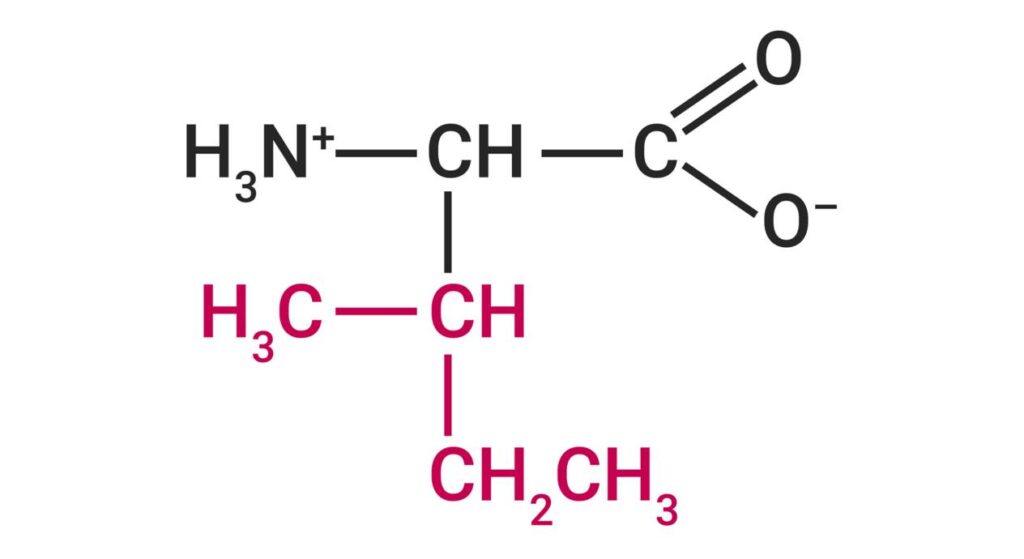
Isoleucine plays important roles in energy production, glucose metabolism, and muscle repair.
Valine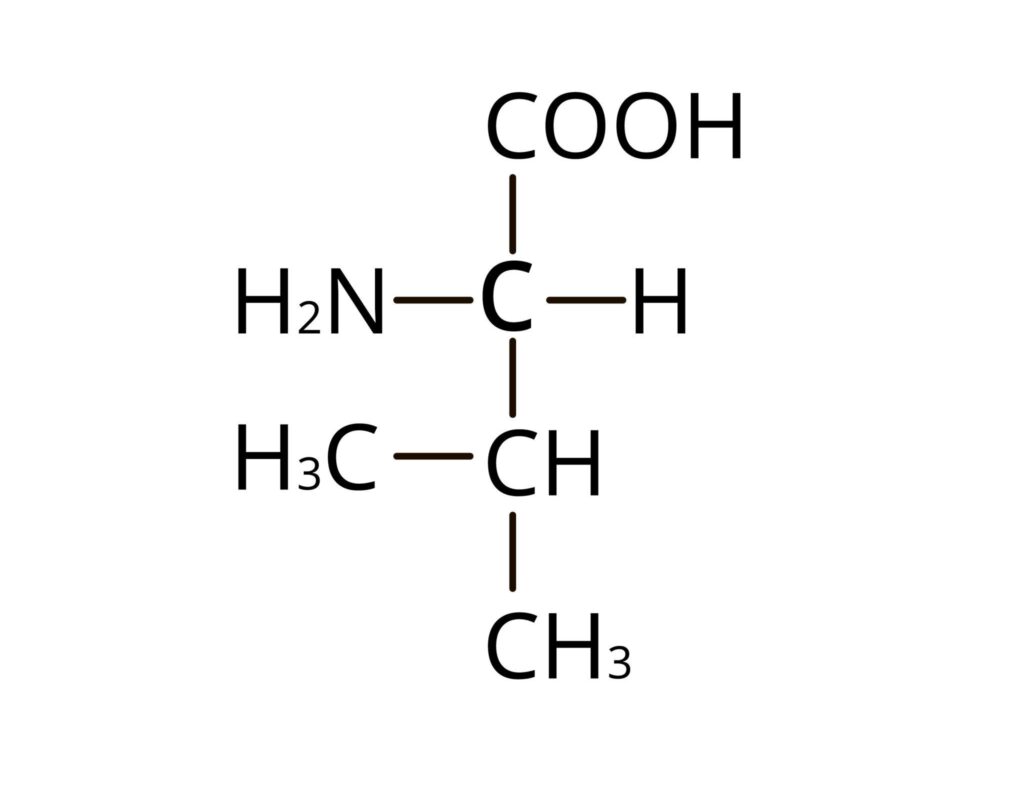
Valine contributes to tissue repair, nitrogen balance, and energy metabolism.
The term “branched-chain” refers to the branched structure of their carbon skeletons, which distinguishes them from other amino acids.
Dietary Sources of BCAAs
Since BCAAs are essential amino acids, they must be supplied through diet.
Major dietary sources include:
Animal Sources
- Milk and dairy products
- Eggs
- Fish
- Poultry
- Meat
Vegetarian Sources
- Soybeans
- Lentils
- Chickpeas
- Kidney beans
- Peanuts
- Nuts and seeds
Because the user is vegetarian, plant-based sources such as soy products, legumes, dairy products, and nuts are particularly important contributors to BCAA intake.
Metabolism
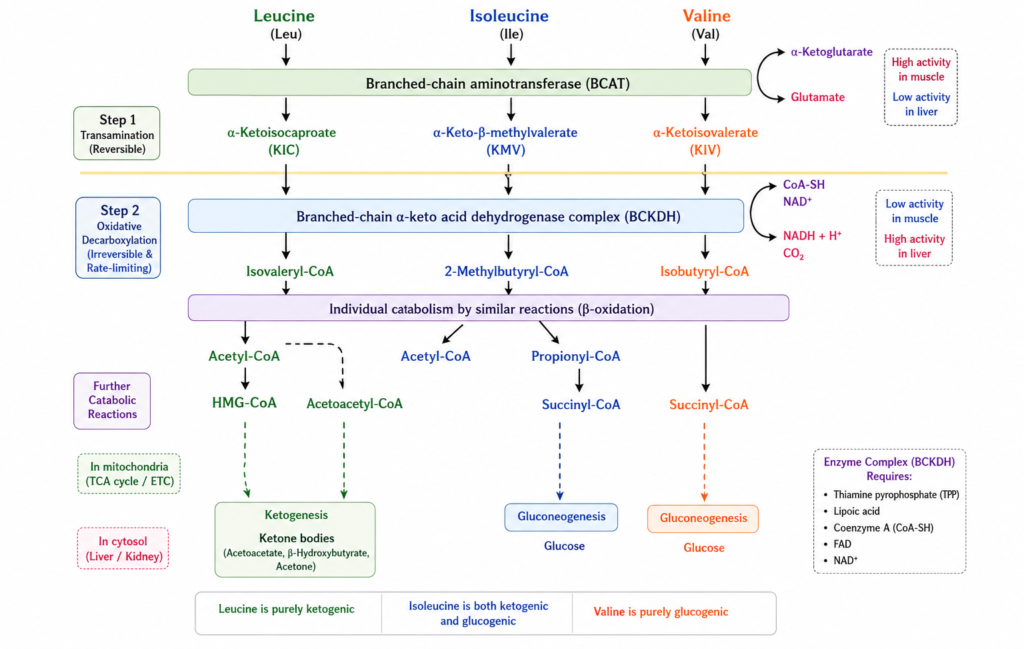
BCAA metabolism occurs through two major enzymatic steps:
Step 1: Transamination
The first reaction is catalyzed by:
Branched-Chain Aminotransferase (BCAT)
In this reaction:
- Leucine → α-Ketoisocaproate (KIC)
- Isoleucine → α-Keto-β-Methylvalerate (KMV)
- Valine → α-Ketoisovalerate (KIV)
The amino group is transferred to α-ketoglutarate, producing glutamate.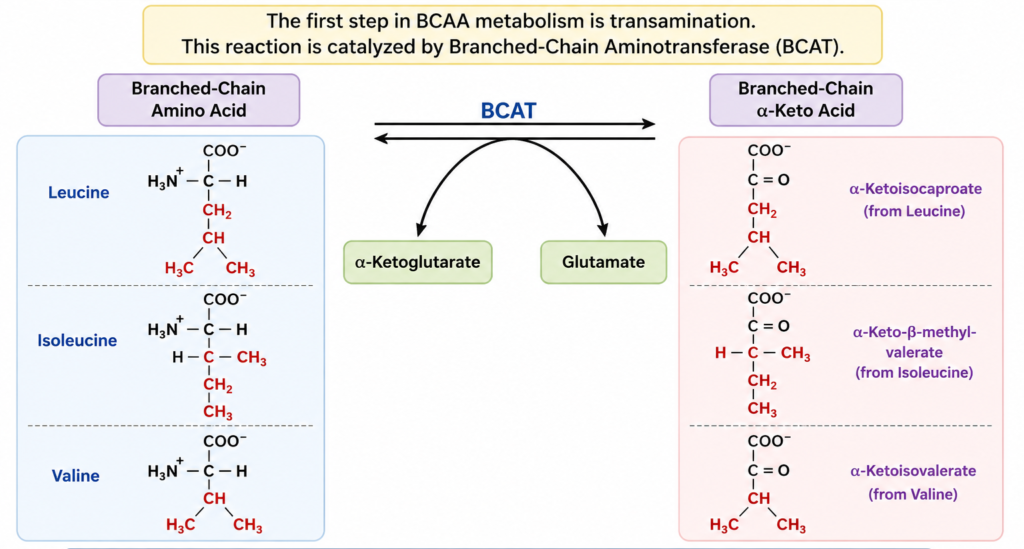
This reversible reaction occurs mainly in:
- Skeletal muscle
- Heart
- Brain
- Kidney
Step 2: Oxidative Decarboxylation
The resulting branched-chain α-keto acids undergo oxidative decarboxylation by:
Branched-Chain α-Ketoacid Dehydrogenase Complex (BCKDH)
This enzyme complex is analogous to:
- Pyruvate dehydrogenase
- α-Ketoglutarate dehydrogenase
The reaction is irreversible and represents the rate-limiting step in BCAA catabolism.
Defects in this enzyme complex result in Maple Syrup Urine Disease (MSUD).
Final Metabolic Products
Each BCAA yields distinct metabolic end products:
Leucine
Produces:
- Acetyl-CoA
- Acetoacetate
Therefore leucine is classified as:
Purely ketogenic
Isoleucine
Produces:
- Acetyl-CoA
- Succinyl-CoA
Therefore isoleucine is:
Both ketogenic and glucogenic
Valine
Produces:
- Succinyl-CoA
Therefore valine is:
Purely glucogenic
These products enter major metabolic pathways such as:
- TCA cycle
- Ketogenesis
- Gluconeogenesis
Physiological Functions of BCAAs
Protein Synthesis
Leucine activates the mTOR pathway, which regulates:
- Muscle protein synthesis
- Cell growth
- Tissue repair
This makes BCAAs particularly important during:
- Growth
- Recovery from illness
- Exercise adaptation
Energy Production During Exercise
During prolonged exercise:
- Glycogen stores decline.
- BCAA oxidation increases.
- Skeletal muscles utilize BCAAs as fuel.
This contributes to maintenance of energy production during endurance activities.
Nitrogen Transport
BCAAs participate in:
- Alanine cycle
- Glutamine synthesis
These pathways facilitate safe transport of nitrogen between tissues.
Immune Function
BCAAs support:
- Lymphocyte proliferation
- Cytokine production
- Immune cell metabolism
Deficiency may impair immune responses.
Regulation of BCAA Metabolism
The regulation of branched-chain amino acid (BCAA) metabolism primarily occurs at the Branched-Chain α-Ketoacid Dehydrogenase (BCKDH) complex, which catalyzes the rate-limiting step in BCAA catabolism.
BCKDH Kinase (BCKDK) – BCKDH kinase phosphorylates and inactivates the BCKDH complex, thereby reducing the breakdown of leucine, isoleucine, and valine.
BCKDH Phosphatase (PPM1K) – BCKDH phosphatase removes the phosphate group from BCKDH, activating the enzyme complex and increasing BCAA oxidation.
Feedback Regulation – The leucine metabolite α-ketoisocaproate (KIC) inhibits BCKDH kinase, resulting in activation of BCKDH and enhanced BCAA catabolism.
Nutritional and Hormonal Regulation
- Fasting and exercise increase BCAA degradation to provide energy.
- High protein intake stimulates BCAA catabolism.
- Insulin promotes protein synthesis and reduces BCAA breakdown.
Clinical Significance
Maple Syrup Urine Disease (MSUD)
- Maple Syrup Urine Disease (MSUD) is a rare autosomal recessive inherited metabolic disorder caused by deficiency of the Branched-Chain α-Ketoacid Dehydrogenase (BCKDH) complex, the key enzyme involved in the metabolism of branched-chain amino acids (BCAAs).
Biochemical Defect
Deficiency of BCKDH prevents the normal breakdown of:
- Leucine
- Isoleucine
- Valine
As a result, these amino acids and their corresponding α-keto acids accumulate in blood and tissues, producing toxic effects, particularly in the brain.
Clinical Features
Symptoms usually appear in the neonatal period and include:
- Poor feeding
- Vomiting
- Lethargy
- Irritability
- Developmental delay
- Seizures
- Neurological deterioration
A characteristic feature is a sweet “maple syrup” or burnt sugar odor of urine, caused by the accumulation of isoleucine metabolites.
Diagnosis
Diagnosis is based on:
- Elevated plasma levels of leucine, isoleucine, and valine
- Increased branched-chain keto acids in urine
- Newborn screening programs
Treatment
Management includes:
- Lifelong restriction of dietary BCAAs
- Special medical formulas
- Monitoring plasma amino acid levels
- Thiamine supplementation in thiamine-responsive cases
- Liver transplantation in severe cases
Clinical Significance
- If left untreated, MSUD can lead to severe neurological damage, intellectual disability, coma, and death.
- Early diagnosis and dietary management significantly improve outcomes.
BCAAs and Diabetes Mellitus
- Branched-chain amino acids (BCAAs)—leucine, isoleucine, and valine—play important roles in energy metabolism, insulin signaling, and glucose homeostasis.
- Recent studies have shown that abnormal BCAA metabolism is closely associated with insulin resistance and type 2 diabetes mellitus (T2DM).
Biochemical Basis
- In individuals with obesity and insulin resistance, BCAA catabolism is impaired, leading to elevated levels of BCAAs in the blood.
- These increased concentrations may interfere with insulin signaling pathways and contribute to metabolic dysfunction.
Clinical Significance
Elevated plasma BCAA levels have been associated with:
- Insulin resistance
- Prediabetes
- Type 2 diabetes mellitus
- Metabolic syndrome
Studies suggest that increased BCAA levels may appear years before the development of overt diabetes, making them potential early biomarkers of metabolic disease.
Mechanism
Impaired BCAA metabolism may:
- Disrupt insulin signaling
- Promote chronic inflammation
- Increase metabolic stress
- Contribute to glucose intolerance
These effects can accelerate the progression of insulin resistance and diabetes.
Clinical Importance
- Monitoring BCAA metabolism may help in the early identification of individuals at risk of developing type 2 diabetes.
- Ongoing research is exploring the use of BCAAs as biomarkers and potential therapeutic targets in metabolic disorders.
BCAAs and Obesity
- Branched-chain amino acids (BCAAs)—leucine, isoleucine, and valine—are closely linked to obesity and metabolic health.
- Numerous studies have shown that individuals with obesity often have elevated circulating BCAA levels, indicating impaired BCAA metabolism.
Biochemical Basis
- In obesity, reduced BCAA catabolism and mitochondrial dysfunction lead to the accumulation of BCAAs in the bloodstream.
- Excess adipose tissue also contributes to metabolic disturbances that affect BCAA utilization.
Clinical Significance
Elevated BCAA levels have been associated with:
- Obesity
- Insulin resistance
- Metabolic syndrome
- Type 2 diabetes mellitus
- Increased cardiovascular risk
Mechanism
Abnormal BCAA metabolism may:
- Impair insulin signaling
- Promote chronic inflammation
- Increase metabolic stress
- Contribute to fat accumulation and metabolic dysfunction
These effects may worsen obesity-related complications and accelerate the development of metabolic diseases.
Clinical Importance
- Because elevated BCAA levels are frequently observed in obese individuals, they are being investigated as potential biomarkers for obesity-related metabolic disorders and early indicators of insulin resistance.
BCAAs and Cardiovascular Disease
- Branched-chain amino acids (BCAAs)—leucine, isoleucine, and valine—have emerged as important metabolic biomarkers in cardiovascular research.
- Elevated circulating BCAA levels have been associated with an increased risk of cardiovascular disease (CVD), particularly in individuals with obesity, insulin resistance, and type 2 diabetes mellitus.
Biochemical Basis
- Impaired BCAA catabolism leads to the accumulation of BCAAs and their metabolites in the bloodstream.
- These metabolic alterations may contribute to endothelial dysfunction, inflammation, and impaired energy metabolism in cardiovascular tissues.
Clinical Significance
Elevated BCAA levels have been linked to:
- Coronary artery disease
- Atherosclerosis
- Hypertension
- Heart failure
- Increased cardiovascular mortality
Mechanism
Abnormal BCAA metabolism may:
- Promote insulin resistance
- Increase oxidative stress
- Enhance inflammatory responses
- Contribute to endothelial dysfunction
- Accelerate atherosclerotic plaque formation
These factors collectively increase cardiovascular risk.
Clinical Importance
- Plasma BCAA concentrations are being investigated as potential biomarkers for early cardiovascular risk assessment and metabolic health monitoring.
- However, further research is needed to fully understand their role in cardiovascular disease development.
BCAAs and Liver Disease
In chronic liver disease:
- BCAA levels decrease
- Aromatic amino acids increase
This imbalance contributes to hepatic encephalopathy.
BCAA supplementation is sometimes used to improve nutritional status and support liver function in selected patients.
BCAAs in Sports Nutrition
BCAA supplementation has become popular among athletes because of potential benefits such as:
- Enhanced muscle recovery
- Reduced muscle breakdown
- Improved exercise performance
- Increased protein synthesis
However, scientific evidence remains mixed, and adequate dietary protein intake often provides sufficient BCAAs.
Emerging Research and Future Perspectives
Recent advances in metabolomics have identified BCAAs as important biomarkers for:
- Metabolic syndrome
- Diabetes risk
- Cardiovascular disease
- Cancer metabolism

