Introduction
- Purine ribonucleotides are essential biomolecules required for the synthesis of DNA, RNA, and many energy-carrying compounds in the body.
- The two major purine nucleotides are adenosine monophosphate (AMP) and guanosine monophosphate (GMP), which are synthesized by specialized metabolic pathways.
- Purine nucleotides are produced by two main pathways: the de novo pathway, which builds the purine ring from simple molecules, and the salvage pathway, which recycles free purine bases.
- The de novo pathway begins with ribose-5-phosphate, which is converted into phosphoribosyl pyrophosphate (PRPP) before the purine ring is assembled.
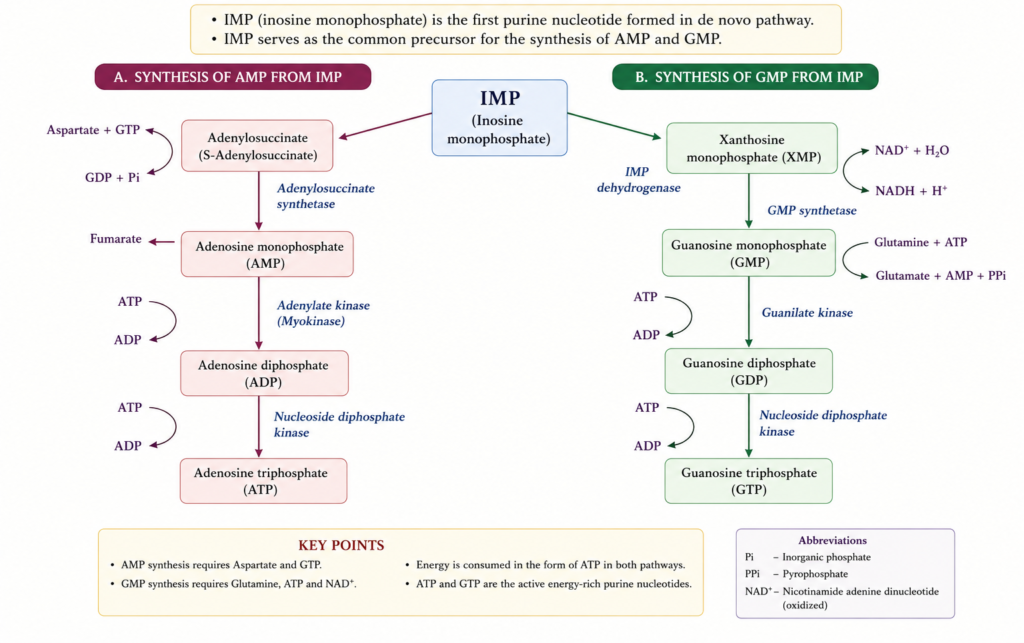
- The first purine nucleotide formed is inosine monophosphate (IMP), which serves as the common precursor for the synthesis of AMP and GMP.
- Purine biosynthesis is a highly regulated process that ensures an adequate supply of nucleotides for cell growth, division, and normal metabolic functions.
Biological Functions
Purine ribonucleotides perform several essential functions in the body. Their major functions include:
- Building Blocks of Nucleic Acids: Purine nucleotides (AMP and GMP) are essential components of DNA and RNA, which store and transmit genetic information.
- Energy Transfer: Adenosine triphosphate (ATP) and guanosine triphosphate (GTP) serve as the primary energy carriers for various cellular processes.
- Cell Signaling: Cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP) act as important second messengers in intracellular signal transduction.
- Components of Coenzymes: Purine nucleotides are present in several coenzymes, including NAD⁺, NADP⁺, FAD, and coenzyme A, which participate in numerous metabolic reactions.
- Protein Synthesis: GTP provides the energy required for the initiation, elongation, and termination steps of protein synthesis.
- Regulation of Metabolism: ATP and other purine nucleotides regulate the activity of many enzymes and metabolic pathways within the cell.
- Cell Growth and Division: Purine nucleotides are essential for DNA replication and RNA synthesis during cell growth, repair, and division.
Classification
Purine nucleotides can be classified based on the nitrogenous base and the number of phosphate groups they contain.
1. Adenine Nucleotides
These nucleotides contain the purine base adenine.
- Adenosine monophosphate (AMP)
- Adenosine diphosphate (ADP)
- Adenosine triphosphate (ATP)
2. Guanine Nucleotides
These nucleotides contain the purine base guanine.
- Guanosine monophosphate (GMP)
- Guanosine diphosphate (GDP)
- Guanosine triphosphate (GTP)
3. Cyclic Purine Nucleotides
These are modified purine nucleotides that function as intracellular second messengers.
- Cyclic adenosine monophosphate (cAMP)
- Cyclic guanosine monophosphate (cGMP)
Cellular Location and Tissue Distribution
Cellular Location
- Purine ribonucleotide biosynthesis occurs mainly in the cytosol (cytoplasm) of cells.
- All the enzymes required for the de novo pathway are present in the cytosol, where the purine ring is synthesized on the ribose sugar.
Tissue Distribution
Purine biosynthesis takes place in most tissues, but it is most active in rapidly dividing cells. Major sites include:
- Liver (primary site of de novo synthesis)
- Bone marrow
- Intestinal mucosa
- Thymus and lymphoid tissues
- Growing and regenerating tissues
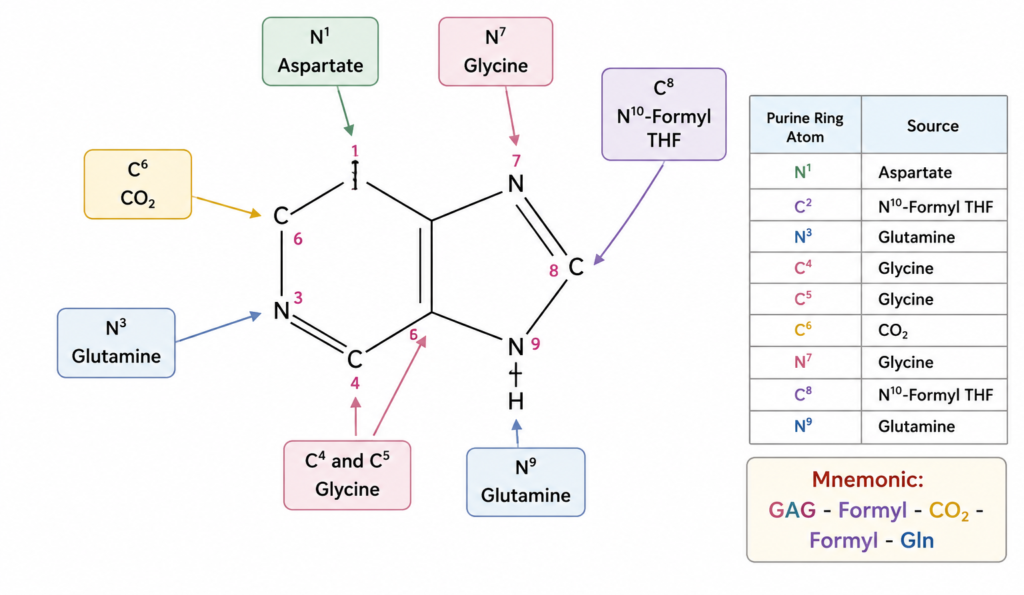
Sources of Purine Ring Atoms
The purine ring is synthesized from several small molecules. Each atom of the ring is contributed by a specific precursor.
| Purine Ring Atom | Source |
|---|---|
| N1 | Aspartate |
| C2 | N¹⁰-Formyl tetrahydrofolate (N¹⁰-formyl THF) |
| N3 | Glutamine |
| C4 | Glycine |
| C5 | Glycine |
| C6 | Carbon dioxide (CO₂) |
| N7 | Glycine |
| C8 | N¹⁰-Formyl tetrahydrofolate (N¹⁰-formyl THF) |
| N9 | Glutamine |
Mnemonic: GAG – Formyl – CO₂ – Formyl – Gln
(Glycine, Aspartate, Glutamine, Formyl-THF, Carbon dioxide, Formyl-THF, Glutamine)
Formation of Phosphoribosyl Pyrophosphate (PRPP)
- Phosphoribosyl pyrophosphate (PRPP) is the activated ribose donor required for the synthesis of purine nucleotides.
- It is the first important intermediate in the de novo pathway.
Reaction
- Ribose-5-phosphate + ATP → PRPP + AMP
- Enzyme: PRPP synthetase (Ribose-phosphate pyrophosphokinase)
De Novo Biosynthesis of Purine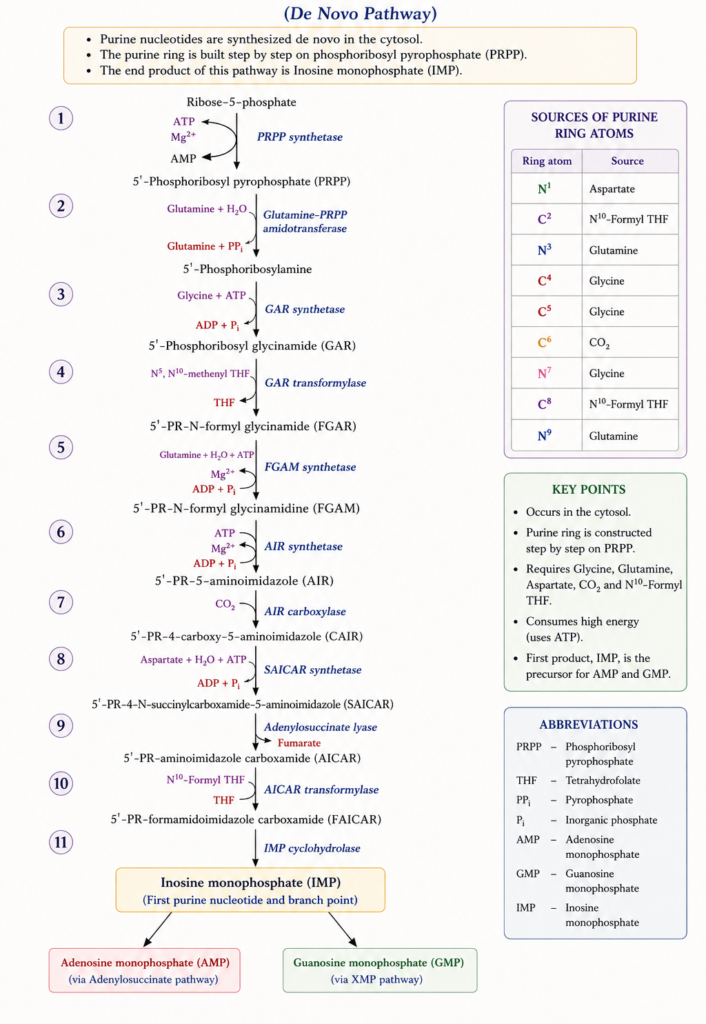
Inhibitors of Purine Synthesis
Several drugs inhibit purine nucleotide synthesis by blocking key enzymes in the de novo pathway. These drugs are used in the treatment of cancer, autoimmune diseases, and infections.
| Inhibitor | Target Enzyme/Action | Clinical Use |
|---|---|---|
| Methotrexate | Inhibits dihydrofolate reductase (DHFR), reducing tetrahydrofolate required for purine synthesis | Cancer, rheumatoid arthritis, psoriasis |
| Trimethoprim | Inhibits bacterial DHFR | Bacterial infections |
| Pyrimethamine | Inhibits protozoal DHFR | Malaria and toxoplasmosis |
| 6-Mercaptopurine (6-MP) | Inhibits de novo purine synthesis by blocking the conversion of PRPP to phosphoribosylamine | Acute lymphoblastic leukemia (ALL) |
| Azathioprine | Converted to 6-mercaptopurine; inhibits purine synthesis | Immunosuppressant in organ transplantation and autoimmune diseases |
| Mycophenolate mofetil | Inhibits IMP dehydrogenase, preventing GMP synthesis | Prevention of organ transplant rejection |
| Ribavirin | Inhibits IMP dehydrogenase, reducing GTP synthesis | Viral infections (e.g., hepatitis C, RSV) |
Synthesis of AMP and GMP from IMP
Salvage Pathway
The salvage pathway is a process by which free purine bases released during the breakdown of nucleic acids are recycled to form purine nucleotides. This pathway is energy-efficient because it reuses existing purine bases instead of synthesizing them from simple precursors.
Major Reactions
| Purine Base | Enzyme | Product |
|---|---|---|
| Adenine + PRPP | Adenine phosphoribosyltransferase (APRT) | AMP + PPi |
| Hypoxanthine + PRPP | Hypoxanthine-guanine phosphoribosyltransferase (HGPRT) | IMP + PPi |
| Guanine + PRPP | Hypoxanthine-guanine phosphoribosyltransferase (HGPRT) | GMP + PPi |
Regulation of Purine Biosynthesis
Purine biosynthesis is tightly regulated to maintain an adequate supply of nucleotides and prevent excessive purine production. The major regulatory mechanisms are as follows:
| Regulatory Step | Enzyme | Activator | Inhibitor | Function |
|---|---|---|---|---|
| 1. PRPP Formation | PRPP synthetase | Inorganic phosphate (Pi) | ADP, GDP | Controls the synthesis of PRPP, the starting substrate for purine biosynthesis. |
| 2. Committed (Rate-Limiting) Step | Glutamine-PRPP amidotransferase | PRPP | IMP, AMP, GMP | Catalyzes the first committed step of de novo purine synthesis; regulated by feedback inhibition. |
| 3. AMP Synthesis | Adenylosuccinate synthetase | GTP | AMP | Regulates the conversion of IMP to AMP and prevents excess AMP formation. |
| 4. GMP Synthesis | IMP dehydrogenase | ATP | GMP | Regulates the conversion of IMP to GMP and prevents excess GMP formation. |
| 5. Reciprocal Regulation | AMP and GMP synthetic pathways | AMP synthesis requires GTP; GMP synthesis requires ATP | — | Maintains a balanced production of AMP and GMP. |
Degradation of Purine Nucleotides
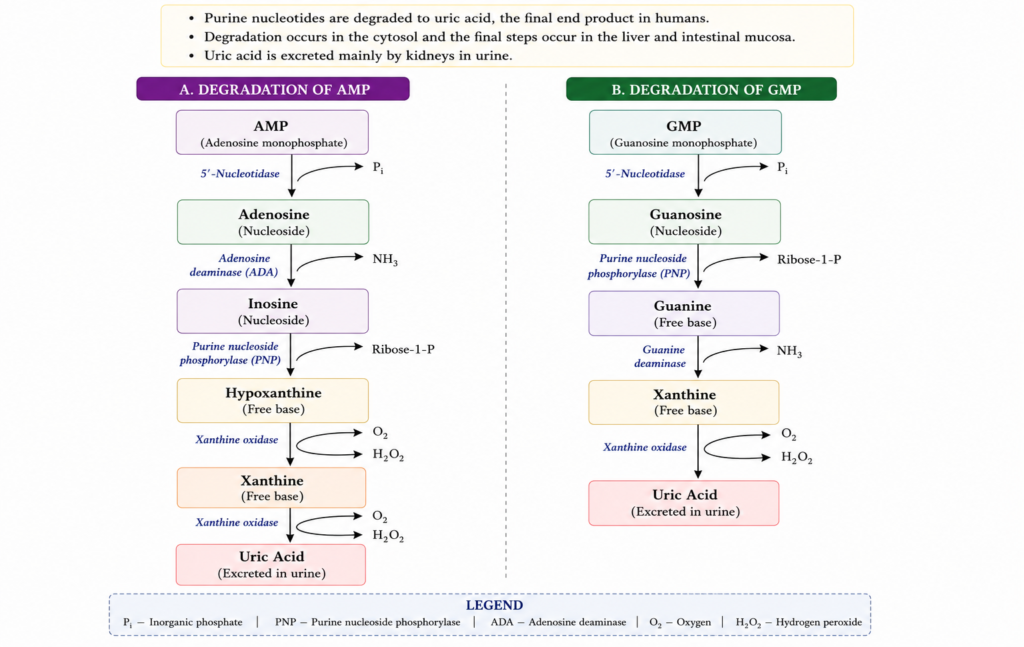
Disorders of Purine Metabolism
Gout
Gout is a metabolic disorder characterized by hyperuricemia (elevated serum uric acid) and the deposition of monosodium urate (MSU) crystals in joints and soft tissues. It is the most common disorder of purine metabolism and causes recurrent episodes of acute inflammatory arthritis.
Causes
1. Increased Uric Acid Production
- Increased de novo purine synthesis
- High-purine diet (red meat, seafood)
- Increased cell turnover (e.g., leukemia, lymphoma)
- Lesch–Nyhan syndrome
2. Decreased Uric Acid Excretion (Most Common)
- Chronic kidney disease
- Diuretic therapy
- Dehydration
- Alcohol consumption
Pathogenesis
- Hyperuricemia leads to the formation of monosodium urate crystals.
- These crystals are deposited in joints, tendons, and soft tissues.
- Crystal deposition activates inflammatory cells, causing the release of cytokines and inflammatory mediators.
- This results in acute pain, swelling, redness, and tenderness of the affected joint.
Clinical Features
- Sudden onset of severe joint pain (often at night)
- Swelling, redness, and warmth of the joint
- Podagra (first metatarsophalangeal joint involvement) is the classic presentation
- Recurrent attacks of arthritis
- Tophi (urate crystal deposits) in chronic gout
- Kidney stones (uric acid nephrolithiasis)
Laboratory Findings
| Investigation | Finding |
|---|---|
| Serum uric acid | ↑ Increased (>7 mg/dL) |
| Synovial fluid | Needle-shaped, negatively birefringent monosodium urate crystals |
| ESR and CRP | ↑ Increased during acute attack |
| X-ray | Tophi and punched-out erosions in chronic gout |
Diagnosis
- Clinical presentation
- Elevated serum uric acid
- Synovial fluid examination showing needle-shaped, negatively birefringent monosodium urate crystals
- X-ray or ultrasound in chronic cases
Treatment
Acute Gout
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Colchicine
- Corticosteroids
Chronic Gout
- Allopurinol (xanthine oxidase inhibitor)
- Febuxostat (xanthine oxidase inhibitor)
- Probenecid (increases uric acid excretion)
- Low-purine diet and adequate hydration
Complications
- Chronic tophaceous gout
- Joint deformity
- Uric acid kidney stones
- Chronic kidney disease
Lesch–Nyhan Syndrome
A rare X-linked recessive disorder caused by deficiency of hypoxanthine-guanine phosphoribosyltransferase (HGPRT).
Cause
- Deficiency of HGPRT (Hypoxanthine-Guanine Phosphoribosyltransferase)
- Inheritance: X-linked recessive
- Gene involved: HPRT1 gene on the X chromosome
Biochemical Defect
- Failure of the purine salvage pathway
- Increased PRPP levels
- Increased de novo purine synthesis
- Excess uric acid production
Clinical Features
- Hyperuricemia
- Gout
- Orange “sand-like” crystals in diapers
- Intellectual disability
- Choreoathetosis
- Self-mutilation (lip and finger biting)
Laboratory Findings
- Increased uric acid
- Decreased HGPRT activity
Treatment
- Allopurinol (reduces uric acid)
- Supportive neurological care
Adenosine Deaminase (ADA) Deficiency
An inherited deficiency of adenosine deaminase (ADA) causing Severe Combined Immunodeficiency (SCID).
Biochemical Defect
- Accumulation of deoxyadenosine and dATP
- Inhibition of DNA synthesis
- Destruction of T and B lymphocytes
Clinical Features
- Recurrent severe infections
- Failure to thrive
- Chronic diarrhea
- Poor immune response
Treatment
- Bone marrow transplantation
- Enzyme replacement therapy (PEG-ADA)
- Gene therapy
Purine Nucleoside Phosphorylase (PNP) Deficiency
A rare autosomal recessive disorder caused by deficiency of purine nucleoside phosphorylase (PNP).
Biochemical Defect
- Impaired degradation of purine nucleosides
- Toxic accumulation of deoxyguanosine
Clinical Features
- Recurrent infections
- T-cell immunodeficiency
- Neurological abnormalities
Treatment
- Bone marrow transplantation
- Supportive therapy
Xanthinuria
A rare disorder caused by deficiency of xanthine oxidase.
Biochemical Defect
- Failure to convert xanthine into uric acid
- Increased xanthine excretion
- Decreased serum uric acid
Clinical Features
- Kidney stones
- Hematuria
- Muscle pain after exercise
- Renal damage (rare)
Treatment
- Low-purine diet
- Increased fluid intake
- Avoid strenuous exercise
Pseudogout (Calcium Pyrophosphate Deposition Disease, CPPD)
Pseudogout is a crystal-induced arthritis caused by the deposition of calcium pyrophosphate dihydrate (CPPD) crystals in joints. It resembles gout clinically but differs in the type of crystals involved.
Pseudogout is an inflammatory joint disorder characterized by the accumulation of CPPD crystals in cartilage and synovial fluid, leading to acute or chronic arthritis.
Causes
- Aging (most common)
- Joint trauma or surgery
- Hyperparathyroidism
- Hemochromatosis
- Hypomagnesemia
- Chronic kidney disease
- Idiopathic (unknown cause)
Pathogenesis
Deposition of calcium pyrophosphate crystals in the joint activates inflammatory cells, resulting in pain, swelling, and stiffness.
Clinical Features
- Sudden onset of joint pain
- Swelling and redness of the affected joint
- Warm, tender joint
- Commonly affects the knee, followed by the wrist, shoulder, ankle, and elbow
- Fever may occur during acute attacks
Laboratory Findings
- Normal or mildly elevated serum uric acid
- Synovial fluid shows rhomboid-shaped, weakly positively birefringent CPPD crystals under polarized light microscopy.
- X-ray may reveal chondrocalcinosis (calcification of cartilage).
Treatment
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Colchicine
- Corticosteroids (oral or intra-articular)
- Joint aspiration to relieve symptoms
- Management of underlying metabolic disorders
Immunodeficiency Diseases Associated with Purine Metabolism
- Purine metabolism is essential for the normal development and function of the immune system.
- Defects in enzymes involved in purine metabolism lead to the accumulation of toxic metabolites, which impair the growth and survival of lymphocytes, resulting in immunodeficiency disorders.
Major Immunodeficiency Diseases
| Disease | Enzyme Deficiency | Biochemical Defect | Immune Cells Affected | Clinical Features |
|---|---|---|---|---|
| Severe Combined Immunodeficiency (SCID) | Adenosine deaminase (ADA) | Accumulation of deoxyadenosine and dATP inhibits DNA synthesis | T cells, B cells, and NK cells | Severe recurrent infections, failure to thrive, chronic diarrhea |
| Purine Nucleoside Phosphorylase (PNP) Deficiency | Purine nucleoside phosphorylase | Accumulation of deoxyguanosine and dGTP | Mainly T cells | Recurrent infections, neurological abnormalities, autoimmune disorders |

