Introduction
- Cardiac Troponin I is one of the most important cardiac biomarkers used for the diagnosis of myocardial injury and acute myocardial infarction (AMI).
- It is considered a highly sensitive and highly specific marker for damage to cardiac muscle cells.
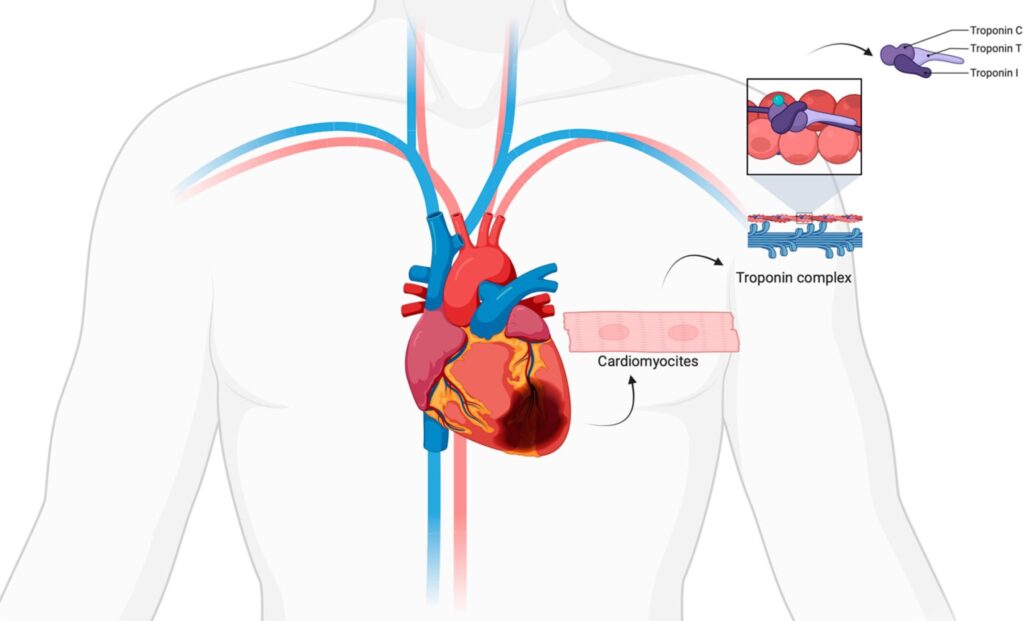
- The troponin complex plays a major role in the contraction of cardiac muscle.
- When myocardial cells are damaged due to ischemia or infarction, cardiac troponin I is released into the bloodstream.
- Detection of elevated cTnI levels, therefore, helps clinicians diagnose acute coronary syndromes accurately and rapidly.
Compared to older cardiac markers such as:
- CK-MB
- LDH
- Myoglobin
cTnI provides:
- Better specificity
- Higher sensitivity
- Longer diagnostic window period
Principle of cTnI Test
The cardiac troponin I test is usually based on:
- Immunochromatographic assay
- ELISA
- Chemiluminescent immunoassay
The test uses monoclonal antibodies directed against cardiac-specific troponin I antigen.
- cTnI present in patient serum binds with specific antibodies
- Antigen-antibody complexes produce measurable signals
- Signal intensity corresponds to troponin concentration
Specimen Required
Common Specimens
- Serum
- Plasma
- Whole blood
Sample Collection
- Venous blood collected aseptically
Testing should preferably be done immediately because the half-life of cTnI is approximately 2–4 hours.
Requirements
- cTnI rapid test cassette/device
- Sample dropper or micropipette
- Assay buffer
- Timer
- Serum, plasma, or whole blood sample
Procedure
1. Preparation
- Bring the test kit and specimen to room temperature before testing.
- Open the test cassette pouch carefully.
2. Labeling
- Label the test device properly with patient identification details.
3. Addition of Sample
- Place the test cassette on a flat surface.
- Add the recommended quantity of sample into the sample well.
Usually:
- 2–3 drops of serum/plasma
or
- 1 drop whole blood + buffer
(Follow manufacturer instructions.)
4. Addition of Buffer
- Add assay buffer into the buffer well if required.
The buffer facilitates movement of the sample through the membrane.
5. Incubation
- Allow the reaction to occur for the recommended time.
- Usually wait:
- 10–20 minutes
Do not interpret results after excessive delay.
Interpretation of Results
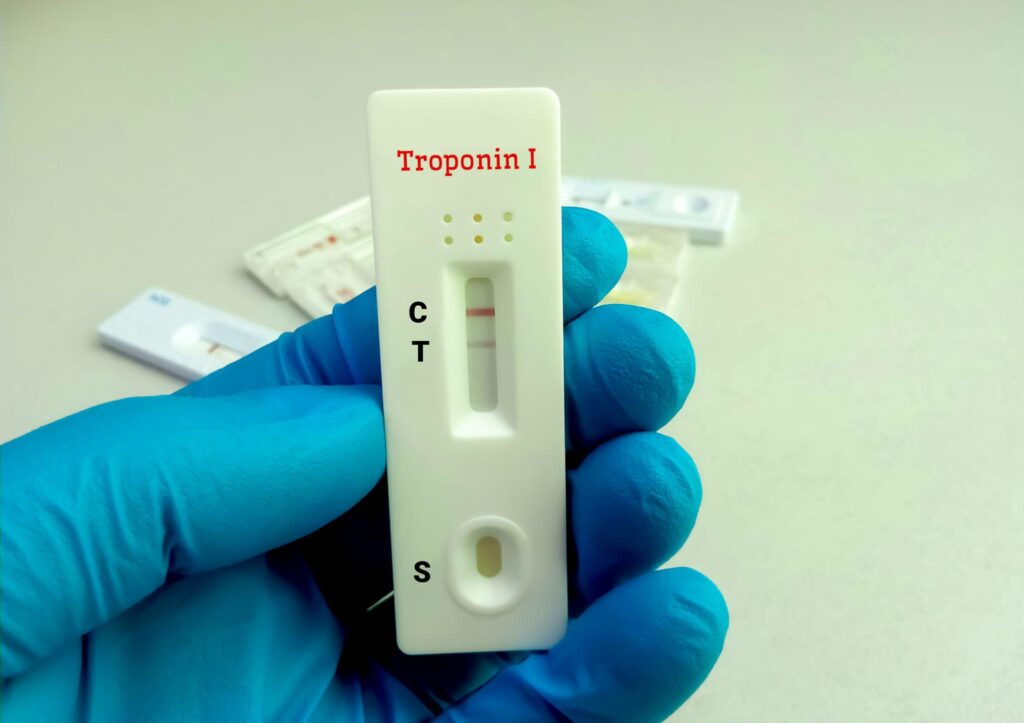
1. Positive Result
- Two colored lines appear:
- Control line (C)
- Test line (T)
Indicates presence of elevated cardiac troponin I.
Suggestive of:
- Myocardial injury
- Acute myocardial infarction
2. Negative Result
- Only control line appears.
Indicates:
- No detectable elevation of cTnI
However, early AMI cannot be ruled out with a single negative test.
3. Invalid Result
- Control line absent.
Possible causes:
- Incorrect procedure
- Insufficient sample
- Faulty test device
Test should be repeated.
Timing of Testing
cTnI levels rise according to time after myocardial injury.
| Parameter | cTnI |
|---|---|
| Initial rise | 3–8 hours |
| Peak level | 12–24 hours |
| Remains elevated | 7–10 days |
Clinical Significance
1. Diagnosis of Acute Myocardial Infarction (AMI)
- Gold standard biomarker for AMI diagnosis
- Highly sensitive and specific for myocardial injury
- Detects even minor cardiac muscle damage
2. Diagnosis of Acute Coronary Syndrome (ACS)
Useful in diagnosis of:
- NSTEMI
- Unstable angina
- Acute coronary syndrome
3. Risk Stratification
- Helps identify high-risk cardiac patients
- Elevated levels indicate poor prognosis and increased mortality risk
4. Detection of Minor Myocardial Damage
- Detects microinfarction and small myocardial injuries
- More sensitive than CK-MB and myoglobin
5. Monitoring Cardiac Patients
Useful in monitoring:
- Cardiac surgery patients
- Angioplasty procedures
- Progression of myocardial injury
6. Elevated in Other Conditions
cTnI may also increase in:
- Myocarditis
- Congestive heart failure
- Pulmonary embolism
- Renal failure
- Sepsis
7. Time Course
- Rises within 3–8 hours after myocardial injury
- Peaks at 12–24 hours
- Remains elevated for 7–10 days
8. Important Clinical Advantages
- Higher specificity than CK-MB
- Better sensitivity for early myocardial injury
- Important test in emergency cardiac diagnosis
- Helps guide treatment decisions in chest pain patients
Advantages
1. High Specificity
- Highly specific for cardiac muscle injury
- Minimal interference from skeletal muscle damage
2. High Sensitivity
- Detects even minor myocardial damage
- Useful for early diagnosis of AMI
3. Long Diagnostic Window
- Remains elevated for 7–10 days
- Useful in late-presenting patients
4. Better Than Older Biomarkers
Superior to:
- CK-MB
- LDH
- Myoglobin
5. Useful in Emergency Diagnosis
- Rapid diagnosis of chest pain patients
- Helps guide immediate treatment
6. Prognostic Value
- Helps assess severity and prognosis of cardiac disease
Limitations
1. Elevated in Non-AMI Conditions
cTnI may also increase in:
- Myocarditis
- Heart failure
- Renal failure
- Sepsis
- Pulmonary embolism
2. Not Useful for Very Early Diagnosis
- May remain normal during first few hours after myocardial injury
- Serial testing may be required
3. Not Ideal for Detecting Reinfarction
- Remains elevated for several days
- Difficult to diagnose reinfarction early
4. Requires Clinical Correlation
- Results must be interpreted with:
- ECG findings
- Clinical symptoms
- Other investigations
5. False Results Possible
Improper sample handling or technical errors may affect results.